
Dr. William Makis is a Nuclear Medicine Radiologist and Oncologist living in Alberta, Canada. Since 2021, Dr. Makis has been voicing concerns about COVID-19 vaccines, vaccine mandates, and the sudden deaths of Canadian doctors and children since the rollout of the mRNA vaccines. He testifies in depth regarding the dramatic deaths of health care professionals and other demographics since the rollout of the mRNA vaccines.
View / Listen: Rumble
[00:01:48]
Shawn Buckley
Good evening and welcome to this special sitting of the National Citizens Inquiry. My name is Shawn Buckley. I’m a lawyer that volunteers at the National Citizens Inquiry, and we’re very pleased to have Dr. William Makis, who will be testifying for the first time at the National Citizens Inquiry.
For those of you who are not familiar with us, we are a citizen-led, a citizen-run, and a citizen-funded group that just decided to appoint independent commissioners and march them across the country. And we basically have created the largest library of under-oath testimony in the world on COVID-19 issues. What’s been accomplished has been absolutely fantastic. But we have some holes in our evidence, including evidence on cancer and some other interesting things that Dr. Makis is going to share with us today.
I guess I will start formally: Commissioners, for the record, my name is Buckley, initial S. I’m attending this evening as agent for the Inquiry Administrator, the Honourable Ches Crosbie.
Dr. Makis, before we begin, can I ask you to state your full name for the record, spelling your first and last name?
Dr. William Makis
My name is Dr. William Makis, V-I-L-I-A-M M-A-K-I-S.
Shawn Buckley
And Dr. Makis, do you promise to tell the truth, the whole truth, and nothing but the truth,
so help you God?
Dr. William Makis
I do.
Shawn Buckley
Now, by way of just some background¬¬— And I will indicate for both the commissioners who have received your CV earlier today and for those that will be watching your testimony that your CV has been entered as Exhibit VT-3 in these proceedings, so everyone can view your expertise. And I will also indicate that every document that you refer to today and the slide presentation that you’re going to use are also entered as exhibits and will be available on your testimony page online.
But briefly, you, in 2001, received a degree in Immunology from the University of Toronto. In 2005, you graduated from the Faculty of Medicine in McGill, but you made a decision to train for five more years at McGill in the area of nuclear medicine to become an oncologist. And that’s what you are: you’re a nuclear medicine radiologist and oncologist. You worked at the Brandon Regional Health Centre, Department of Nuclear Medicine, and then more recently at the Cross Cancer Institute, Department of Diagnostic Imaging in Edmonton.
Now, we’ve asked you to testify on a number of topics today, including your experience with vaccine mandates in Alberta, with sudden deaths involving doctors—which you’ve been a pioneer in bringing attention to that. We want you to also share with us about the Alberta government deleting COVID-19 vaccine data from,
[00:05:00]
basically, the public website that they run. We want you to speak about the relationship, if any, between COVID-19 mRNA vaccines and cancer, and then also about sudden deaths and cancer.
So, Dr. Makis, I invite you to begin. You have a presentation for us [Exhibit VT-3a], and then, just as needed, I’ll interrupt you to clarify and ask some questions.
Dr. Willliam Makis
Thank you very much.
I started raising concerns about COVID-19 vaccines on social media in August of 2021 [Exhibit VT-3b]. And it was at this time that Israel had just rolled out booster shots for its population. It was the first country that had rolled out COVID vaccine booster shots. And in my estimation, this was already an indication of failure of the first two doses of the COVID vaccines. Israel rolled out the boosters in people ages 60 and above, then 50 and above. And by the end of August of 2021, it was the country that had the highest COVID-19 infection rate in the world.
And it was right around this time that Alberta Health Services [AHS] announced that it was going to implement a vaccine mandate on all of its 105,000 health care workers. This was the announcement that Alberta Health Services had put out [Exhibit VT-3c]. And the announcement was really unilateral by AHS. There seemed to be no involvement of the Alberta provincial government, Jason Kenney’s government.
It was announced by AHS president and CEO Dr. Verna Yiu. And the announcement stated that immunization against COVID-19 is the most effective means to prevent the spread of COVID-19 and that any AHS employee unable to be immunized due to a medical reason or a protected ground under the Alberta Human Rights Act would be reasonably accommodated. This announcement was carried in a number of mainstream media outlets [Exhibits VT-3d to VT-3g] and one of these was the Calgary Herald [Exhibit VT-3d]. And I just wanted to bring this up—a statement from the Alberta Health Services CEO, Dr. Verna Yiu, stating that she is confident that most health care workers will want to get vaccinated and that if someone refuses and doesn’t have a valid exemption that AHS officials would meet with them to discuss it and, quote, “provide educational resources,” end quote. But that if this re-education was unsuccessful the employees would then be put on unpaid leave of absence.
I became involved at this point. There was tremendous opposition among Alberta health care workers to these COVID vaccine mandates. And there was an open letter that was authored and signed by over 3,500 Alberta health care workers. And I was one of those signatories. Seventy-three other physicians co-signed this letter, and it was then signed by nurses and other health care workers. This is an open letter to the president and CEO, Dr. Verna Yiu, and it outlined the reasons why Alberta health care workers, thousands of them, were opposed to COVID-19 vaccine mandates at this time.
I would like to highlight some of these. First of all, these mRNA vaccines had not been proven to prevent disease uptake or disease transmission. This was supported by the CDC’s own data. The overall survival rate from COVID was approximately 99.7 per cent. The vaccine was already showing weakened efficacy after only a few months. Very importantly, United Kingdom and Israel, two highly vaccinated countries, had very high percentages of hospitalized patients who were fully vaccinated. Natural immunity was superior to vaccine immunity. And many health care workers, you know, had COVID already, had recovered, and already had natural immunity.
And the VAERS database at the time—this is the Vaccine Adverse Event Reporting System—this is as of August 27, 2021, had shown 650,000 people had been injured and 13,900 people had died soon after the administration of the vaccine. And we know that the VAERS reporting system has an underestimation factor of anywhere from 10- to 100-fold. So these numbers were much, much higher.
As health care workers, we believed that the vaccine mandate was contrary to
[00:10:00]
sections two and seven of the Canadian Charter of Rights and Freedoms. And so this letter respectfully requested that the vaccine mandate be rescinded immediately so that Alberta health care workers could continue to provide care for Albertans. This letter was sent to senior officials at Alberta Health Services. One of them was Dr. Francois Belanger, who is the Alberta Health Services vice president and chief medical officer. So he is the lead doctor in the province. It was also sent to the leadership of Covenant Health, which is a smaller health authority in Alberta.
It was signed by 3,544 health care workers, including 73 physicians, and I was one of those physicians.
Shawn Buckley
So can I just stop you, Dr. Makis? So I’m not aware of any other time in history where literally 3,500 health care professionals in Alberta would sign a letter to senior health officials. Are you aware of this ever happening before on any other issue?
Dr. William Makis
I’m not.
Shawn Buckley
And what was the response from these six senior health officials that the letter was sent
to?
Dr. William Makis
As far as I know, there was never any response from Alberta Health Services.
However— So I signed the letter and I was very surprised to receive a letter about three weeks later from the College of Physicians and Surgeons of Alberta [Exhibit VT-3h]. And the College indicated to me that they had received a copy of this letter to Alberta Health Services regarding opposition to mandatory COVID vaccination for AHS employees. And they said, “You have been identified as a signatory on this letter.” The College then says that it is their standard practice to maintain a copy of this on my record, on my permanent record at the College. And then a very interesting paragraph at the end—because they said that they’ve been made aware that some people who had signed the letter actually didn’t agree to sign it or were not aware that their signature was on it and that if I personally did not agree to be a signatory on this letter that I should let the College know and then they would put that response on my permanent record as well. I took this—
Yes, go ahead.
Shawn Buckley
I was just going to ask you: How did you take this? Because it sounds pretty threatening.
Dr. William Makis
Well, I honestly took this letter as a threat. I took it as a threat on my medical licence and, really, on my medical career.
Now, I’d like to point out that there is no patient care issue here. So the College has jurisdiction, obviously, over patient care issues, licensing issues. You know, I had co-signed a letter in opposition to vaccine mandates that I felt were unethical, unscientific, abusive, and harmful. And, you know, I did not see a role for the College to put that letter on my record and then send me an intimidating letter like this.
So it is my understanding that the College probably sent this threatening letter to all 73 Alberta doctors who had co-signed the letter in opposition to the vaccine mandates. And, you know, I don’t know what the other colleges did, like the nursing college, but, you know, I was very concerned to have been sort of implicitly threatened in this way.
Shawn Buckley
So I just want to be clear. So we have 3,544 health care workers sign a letter, citing specific concerns about the mandate, and there’s no response by the four people that are basically heads of health authorities within the province of Alberta. But we have regulatory colleges, who the letter was not addressed to, responding, at least to doctors.
Dr. William Makis
Yes.
Shawn Buckley
Okay.
Dr. William Makis
And so, you know, I remain opposed to vaccine mandates to this day: I was opposed then and I’m still opposed now. I believe they’re very harmful and that remains my stance to this day.
Shawn Buckley
It’s quite fascinating. Now, you’re moving now to doctor deaths, and I can tell you that I’m particularly interested in this one. So please proceed.
Dr. William Makis
This is a phenomenon— These sudden deaths of Canadian doctors was a phenomenon that I have been warning about since December of 2021.
[00:15:00]
And you will see this is my first post on the matter back in December of 2021 on Twitter. And the way I came to this topic and this phenomenon was there were two Canadian doctors—young Canadian doctors—who had died suddenly after taking the booster shot.
And the first of these doctors was Dr. Sohrab Lutchmedial. This was a 52-year-old interventional cardiologist from New Brunswick. Now he was one of the first doctors in Canada to take the COVID vaccine booster shot. He took his shot on October 24th, 2021. He described it on Facebook. He says, “Vax Shot Three: Electric Flu-Galoo.” I’m assuming that he had some flu-like symptoms after he took the shot and people were asking him, “Is this the booster for health care workers?” He says, “Yes, exactly.” And two weeks after he took the booster shot, he died in his sleep on November 8th, 2021.
And Dr. Lutchmedial was a very outspoken critic of people who didn’t want to get vaccinated. And he made a number of Twitter posts that were controversial. I included some of them on this slide. In one of them, he says, “I think all of us would treat the unvaxxed patient with respect and to the best of our abilities, but the people that convinced them not to get vaxxed, I want to punch those people in the face.” There was another post where he stated, “For those who won’t get the shot for selfish reasons, whatever, I won’t cry at their funeral.”
So I was aware of these posts, and then when he took his booster shot, died suddenly. I was very interested in what had happened to this young doctor.
The second doctor who died suddenly, very shortly after, on December 23rd, 2021, it was Dr. Neil Singh Dhalla. This is a family doctor in Toronto, Ontario, who ran clinics called Activa Clinics. And he took his booster shot. And three or four days later, he was at a friend’s Christmas party, felt unwell; he lied down on the couch, and he died suddenly while sleeping on that couch. He died on December 23, 2021.
And there was a TikTok video that had been put out by a friend who said, you know, “He just had his booster shot three or four days ago and this is what happened. He died suddenly a few days later.” There were claims that there was an autopsy showing myocarditis. I was never able to verify that claim.
And so when these two doctors had died suddenly, I realized something was very wrong. There was that temporal association with the booster shot—dying very shortly after the booster shot—and dying in their sleep, which is extremely rare: highly unusual for a young person to die in their sleep. And so I began posting about this on Twitter, and I was trying to alert some doctors about this.
Dr. Irfan Dhalla, who is a very prominent doctor in Toronto, he talked about the risk of booster shots. He made a post in January of 2022. He said, there’s a “huge gap between what scientists and health care workers think [about] the risk of boosters being close to zero long-term risk and what the public thinks.” I responded. I said, “Not true—the long-term risks remain unknown.” And look, there’s these two doctors that died shortly after their booster shots.
I continued trying to raise the alarm on Twitter. Unfortunately, a couple of months later, I was raising concerns about COVID vaccines in children five to eleven years old and my Twitter account was locked, and I was censored and terminated from Twitter. And so I continued doing research on my own, but again, I could not really alert anybody. And so I simply continued looking into the sudden deaths of Canadian doctors. And that’s how this whole thing started for me.
Once I had found 32 sudden deaths of Canadian doctors, I decided to contact the authorities. And I wrote a letter to the Canadian Medical Association on September 3rd of 2022 to their president, Dr. Alika Lafontaine—who was the current president at the time—and Dr. Katherine Smart, who was the previous president for the previous year [Exhibit VT-3i]. I also sent copies of this letter to Alberta Premier Jason Kenney and Alberta Minister of Health Jason Copping.
And I raised concerns about these sudden deaths of 32 young Canadian doctors. I attached photos and information about them. And I said, “Look, these doctors died suddenly or unexpectedly in the past 16 months. They were double, triple, or quadruple COVID-19 vaccinated.” I said that each of these deaths is suspicious for COVID vaccine injury
[00:20:00]
as these previously healthy doctors died suddenly while engaging in regular physical activity. They died unexpectedly in their sleep. They suffered heart attacks, strokes, unusual accidents, or developed sudden-onset aggressive cancers. And I was not familiar yet with the term “turbo cancer” at the time, but I had noticed that some of these doctors suffered very aggressive, unusual cancers.
And I asked the Canadian Medical Association and the presidents to use their platform to publicly call for the immediate termination of COVID vaccine mandates in Canada’s healthcare and to call for urgent investigations and public inquiries into what was killing young, COVID-vaccinated Canadian doctors.
I did not receive a response to this letter from the Canadian Medical Association or from the Alberta Premier and Alberta Minister of Health.
At this time, there was a group of people who had contacted me privately and they said, “Look, we’re willing to offer our services, our time, to help you build a database of all Canadian doctor deaths going back several years so that we could compare and see if doctors were dying at a higher rate than normal, or if this was just some kind of an aberration and was not a real phenomenon.” And so we put a team together and we started assembling this database and, about a month and a half later, our group of sudden deaths had grown to 80.
And so I sent another letter to the Canadian Medical Association [Exhibit VT-3j]. And I said, “Look, I’m providing you an update. Now it’s 80 young doctors who have died suddenly or unexpectedly since the rollout of the vaccines.” And I specify, I say, “Look, you cannot continue ignoring this. My team has assembled a database of 1,638 Canadian doctor deaths during the period of 2019 to 2022.” And we had actually obtained a lot of this data from the Canadian Medical Association’s own website: 972 entries of those were from the CMA’s own website.
And I gave some statistics that the deaths were actually clustered around the young doctors. It was the young doctors who were dying at much, much higher rates than previously. At the time, doctors under the age of 30, it was looking like they were dying at an eight-fold rate higher in 2022 compared to the pre-vaccine rollout era. And I also made a note of young McMaster University medical residents: three of them had died suddenly in the summer of 2022. And I said, “Look, I’d never heard of anything like this in my career; this is unprecedented.” And I once again asked, “Please call for the suspension of vaccine mandates and for investigations.”
These are the three young McMaster residents who died suddenly in the summer of 2022. And look at their ages: Dr. Satyan Choudhuri, 25 years old, family medicine resident. Dr. Candace Nayman, 27 years old, pediatrics resident. Dr. Nayman was a triathlete, and she had actually participated in a triathlon that summer, and she collapsed during the swimming portion of the triathlon, and then died several days later. And Dr. Matthew Foss, 32-year-old anesthesiology resident who struggled with a very aggressive lymphoma.
I attached pictures and information of 80 Canadian doctors’ sudden deaths. And I just wanted to bring up a few of those, if I may?
Shawn Buckley
Yes, please do.
Dr. William Makis
Just to highlight some of these sudden deaths.
Dr. Carl-Éric Gagné is a cardiologist from Trois-Rivières, Quebec, 56 years old, an avid cyclist. He was participating in a 100-kilometre cycling competition. He collapsed during the cycling event, and he died suddenly at the age of 56.
Dr. Paul Hannam, a 50-year-old emergency physician from Toronto. He’s actually an Olympic athlete—an Olympian who went out for a jog. He collapsed while he was jogging, and he died suddenly during his jog.
Dr. Baharan Behzadizad was a 43-year-old family doctor from Newfoundland. She died in her sleep with no explanation.
Dr. Joshua Yoneda, 27-year-old medical student from UBC (University of British Columbia). He was mandated to take two COVID vaccines. A few months later, he develops back pain. It’s discovered he has an extremely aggressive spinal cord tumour, and he died less than one year after diagnosis.
Dr. Bradley James Harris, a 49-year-old family doctor from Comox, BC, was out for a jog. He collapsed while he was jogging. He died suddenly.
Dr. Michael Stefanos, a radiologist from Mississauga, Ontario, 50 years old, died in his sleep.
Dr. Oliver Seifert, 58-year-old family doctor from Edmonton, again, died in his sleep.
[00:25:00]
Dr. Johannes Giede was a psychiatrist, 59 years old, from Prince George, BC. This is an interesting story because his son came out publicly, and he said, “My father had the booster shot.” And a few days later, he started having stroke-like symptoms. And about a few weeks after that, he had a massive stroke, which was fatal. He died from that stroke.
There’s a number of doctors who died after very brief illnesses.
Dr. Jun Kawakami, 48-year-old urologist from Calgary, died from a very, very aggressive pancreatic cancer.
Dr. Au, 53-year-old internist and geriatrician from Edmonton, Alberta. He was very athletic. He would go jogging every single morning and he would try to get his health care colleagues to go jogging with him every single morning. He died of a sudden cardiac vascular event.
Dr. Ainsley Moore, 57-year-old family physician from Hamilton, Ontario, died of a heart attack.
Dr. Inderjit Jassal, 42-year-old family physician from Surrey, BC, collapsed and died unexpectedly from a heart attack.
Dr. Mohammad Alam, 55-year-old family physician from High River, Alberta, had his first COVID vaccine, and he died within 24 hours of his first COVID vaccine.
Dr. James Tazzeo, 51-year-old family physician from Orillia, Ontario, died while he was cross-country skiing.
And so, you know, I gave all this information to the Canadian Medical Association.
Shawn Buckley
Dr. Makis, before you go on, I’ll just let the commissioners know that your entire database, you’ve been gracious enough to share with us, and we have entered that as Exhibit VT-3m.
Dr. William Makis
Thank you.
And so, you know, I received a response that I really didn’t expect. And these responses were in the form of personal attacks against me on social media.
The initial attacks came from a family physician in Ontario, Dr. Michelle Cohen, and she would refer to my database and my information as a “fake Canadian doctor vaccine death story.” And so I included a number of posts here from Dr. Cohen that she made after my first letter to the CMA and after my second letter to the CMA as well. “The fake Canadian doctor vaccine death story continues to circulate.” “This fake number keeps rising.” So she’s referring to the time when the doctor deaths went from 32 to 80. “We’ve gone from ‘a few doctors died around the same time’ to ‘all doctor mortality is vaccine murder.’ What a journey.” And so there’s a certain element of mockery in these posts. Another post: “It’s easy to ridicule a conspiracy theory as absurd as one that claims all Canadian doctor mortality is vaccine murder.” I never made any such claims.
Shawn Buckley
Now, Dr. Makis, did Dr. Cohen ever contact you to ask you about your data, maybe to get your— Basically relating to her what you were relying on and maybe even get a copy of the database that you were accumulating?
Dr. William Makis
Dr. Cohen never asked for this data.
Shawn Buckley
Okay, so you’re being criticized without your data being looked at.
Dr. William Makis
That’s right.
Shawn Buckley
Okay.
Dr. William Makis
And then another post: “The made-up number of Canadian doctors killed by COVID vaccines is now increased to 80.” So now this is a made-up number.
Now, this is the only response that has ever been made by the Canadian Medical Association to my letters [Exhibit VT-3n]. And you can see it’s not addressed to me; it’s actually addressed to Dr. Cohen. And this was on October 20th, 2022, and the Canadian Medical Association actually quotes one of Dr. Cohen’s posts, and it’s a post with the pictures of the doctors who had died with a big red X crossed over their pictures. And the Canadian Medical Association says, “Thank you, Dr. Cohen, for standing up to disinformation. There’s no evidence supporting the various theories that have been circulating. We encourage all Canadians to be up to date with all their vaccines to prevent serious health issues.”
This is the only time that the Canadian Medical Association responded to my information. And you could see they’re putting a picture, again, with a big red X across the pictures of deceased doctors.
Shawn Buckley
Now, you know what, can I just interrupt?
One thing that I find interesting about this is, pre-COVID, my understanding is, basically, there would be a problem with people running around doctors. Whether or not you take a vaccine is something that I used to think you would get your doctor’s advice on. Like this is an experimental treatment. There’s nobody can hide the fact that at the time that this is written,
[00:30:00]
really there was not any long-term or even medium-term data. And so it’s interesting that here we have the Canadian Medical Association excluding doctors: just “we encourage all Canadians to be up to date.” It’s not that they’re saying we encourage all Canadians to seek their doctor’s advice as to whether or not they should get vaccinated.
Does that not strike you as odd, as a physician: that they’re basically doing an end run around their own members when the safest thing is for people to get the advice, for them, from a qualified doctor?
Dr. William Makis
It is strange and, I’ll be honest, the reason why I included, personally, my letters addressed to the presidents of the Canadian Medical Association—Dr. Alika Lafontaine; Dr. Katherine Smart—is because on their personal accounts, they were also encouraging people to get vaccinated.
One of the past presidents, Dr. Gigi Osler—who has been appointed to the Canadian Senate by Prime Minister Justin Trudeau recently—she was putting out pictures of having her daughter vaccinated with the Moderna vaccine. And she said, “Look, go get the Moderna vaccine,” specifically. “I can tell you where you can get those appointments,” and so on. So these individuals were, you know, very personally involved in recommending the vaccines.
One thing I would like to bring up with the Canadian Medical Association, another thing they said was that the In Memoriam service that the Canadian Medical Association offers to members to keep track of their colleagues and recognize their passing— Now this is an In Memoriam page on their website. And so they hosted this In Memoriam section on their website for many years, and it had thousands of doctor deaths, and this was a way to honour doctors who had died. And so they said, “Look, this is provided based on information sent to the Canadian Medical Association and should not be viewed as evidence to support theories surrounding COVID vaccines and other issues.” And I gave a picture of what the In Memoriam page looked like.
Now, around this time, the Canadian Medical Association began deleting data from this In Memoriam website. They began deleting the doctor entries—the doctor deaths—and we had noticed this. We had downloaded all the data, but as we were trying to get some of the previous years, we noticed that the Canadian Medical Association had started to delete this data. And eventually they deleted all the data from 2021 and prior, and they just left the 2022. And then by the end of the year, they deleted that as well.
And so I can tell you that we have a record of about 1,200 doctor deaths that we saved from their website but which they have since deleted. And so these entries are in the database that I’ve provided to the NCI [National Citizens Inquiry].
Shawn Buckley
It’s interesting because— And you’re going to go on to basically— How you were continually attacked about this. But we keep hearing about, you know, data disappearing or it being made very difficult.
We had witness after witness, Dr. Makis, testify—both professional and lay—on how it was near impossible to get an adverse reaction report actually filed with Health Canada. And the funny thing was, pre-COVID, citizens could file adverse reaction reports, but that was taken down pre-COVID. It’s now back up because an access to information request was embarrassing them.
But it’s just interesting that here we have one of the responses to you talking about doctor deaths is the medical association dropping that from their website.
Dr. William Makis
Yes. So, you know, we downloaded all the data from 2019 to 2022 because that was the only time period we were looking at. There were probably earlier entries that were deleted that we didn’t save. But it was about 1,200 entries that we saved that the Canadian Medical Association subsequently deleted. And that website is no longer there. It might be accessible through the Wayback Machine, but they deleted all of it.
Now, shortly after I sent my letter about the 80 Canadian doctor deaths, I was attacked in a fairly coordinated mainstream media campaign and it was started by the Toronto Star [Exhibit VT-3p]. And the story that was put out by the Toronto Star was titled, “Why Won’t a Debunked Conspiracy Theory About Doctors Harmed by the COVID Vaccine Go Away?” And in this Toronto Star piece, they featured this gentleman: Mr. Timothy Caulfield.
[00:35:00]
And at the bottom it says, Mr. Caulfield is the Canada Research Chair in Health Law and Policy at the University of Alberta. It says, “It’s ‘amazing’ how the doctor conspiracy lives on ‘as it was immediately debunked.’”
I had really not heard of Mr. Timothy Caulfield. He did not contact me before putting out the story, and so I really don’t know what kind of debunking the Toronto Star is referring to here.
Shawn Buckley
So, Dr. Makis, can I ask—because you’re going to explain that you were attacked a little more broadly than this—did anyone who attacked this doctor story ever contact you to have you share your actual data with them?
Dr. William Makis
I was contacted by two journalists, and I will mention that as I go through my presentation. But when I was contacted by those journalists—one was from Global News and the other one was from Reuters—they really contacted me with accusatory language right from the beginning, and they didn’t ask to see my data. They said, you know, “You’re lying. You’re causing harm to families. Why are you causing harm to families?” This is the kind of language that I was approached with.
Shawn Buckley
Can I just add, because this is important and I want to make sure that your evidence is clear. So as a medical doctor, you didn’t go looking for researching this. But you saw a couple of doctors had died suddenly and you became concerned, and so you started looking into it and then you basically had a team doing research.
And, I mean, you’re a researcher. I’m just going by memory, but I think your CV lists 105 peer-reviewed published articles that you were an author in. I mean, you understand research, and you understand data needing to be correct. I mean, you do this wrong once, and your reputation is gone.
So you’re looking into doctor deaths.
Dr. William Makis
Yes.
Shawn Buckley
And you’re doing it in a robust way, and you’re being attacked by the media, and not a single journalist or detractor asks to look at the data?
Dr. William Makis
No. And, you know, honestly, I’ve really been shocked at how this was approached by the media. And as I walk through some of these slides, you know, I think it’ll become clear what the intent of the media was. It was not to, certainly, you know, look at the data themselves or look at what the real evidence is. It was, well— Let me move to the next slide.
I wanted to highlight some of the parts of the Toronto Star story. And Mr. Caulfield, who works at the University of Alberta—as I did—he said, “It’s in my social media feed almost every day, if not every day. My hate mailers are emailing this to me,” said Mr. Timothy Caulfield. So right there he’s already coding it in a language of hate.
He says, “One of the things that’s fascinating is that it was immediately debunked in the sense of ‘No, this is wrong, this is actually how these individuals passed away.’ But that didn’t kill the story.” And I think, again, here it sort of shows that—what is the intent? The intent here is to kill the story; it isn’t to learn what the truth is.
“It’s amazing how it won’t die—and it’s amazing the impact it continues to have.” These are quotes from Mr. Timothy Caulfield.
Then the Toronto Star goes on to say, “To be clear, experts are united on the fact”—and I don’t know who these experts are—“that this is a conspiracy theory. The causes of death were well-documented by family in news stories and obituaries. It’s not clear when they were vaccinated, and besides which, their symptoms do not match what we know about vaccine side effects from studies on millions of people.” So now they’re claiming that the obituaries had symptoms and there’s studies on vaccine effects on millions of people? This is outright lying from the Toronto Star.
And interestingly, the Toronto Star now brings in Dr. Michelle Cohen, who had previously attacked me on social media saying that it was fake—it was a fake story; it was a made-up number—and she makes a couple of comments in this story as well. Dr. Cohen [sic] [The Toronto Star] says, it’s “a particularly potent bit of misinformation, says Dr. Michelle Cohen, family doctor in Brighton, Ontario, who has been tracking the advance of the theory since summer. If you already believe that doctors are lying about the safety of vaccines, there is a ‘dark joy’ in the idea that those same health care professionals are being harmed, she argues.”
I can tell you there’s no dark joy in this at all, and this was highly offensive when I read this.
[00:40:00]
“The CMA does not note a connection between vaccines and sudden deaths.” The CMA is quoted as saying, “‘There’s no evidence to confirm or support the various theories that have been circulated,’ the CMA said in an email. The organization ‘is concerned with misinformation and conspiracy theories spreading online about the recent deaths of physicians across the country.’”
Now, the Canadian Medical Association had not responded to my letter, had not asked to see my database. So they are responding without really having contacted me at all.
Shawn Buckley
You know, another interesting thing about this is, it would seem to me that if, you know, you’re right—and I know that A, you’ve shared your database, and B, you’re going to show us some of the actual figures—is you would think that both the media and the College of Physicians and Surgeons would be extremely interested in looking at your data and actually looking into the issue. Because if doctors are being harmed, then you would think that’s the one group we need to protect. Because if the rest of us are in a world of hurt in this pandemic and what’s appearing—starting to come from the data you’re sharing—is vaccine injury, we need the medical professionals to be healthy. Like, that’s the one group we need to protect.
So that’s what I find interesting—is I would just assume that everyone would have been contacting you to verify your data out of concern that you would be right.
Dr. William Makis
I would think the only way to debunk—and they keep using this word “debunk”—would be to look at my data, have data analysts analyze it, and come out and say, “Look, there’s nothing in this data; there’s no evidence.” But they’re saying that there’s no evidence without looking at any of the data.
And as I stated earlier, the majority of the data is taken from the Canadian Medical Association’s own website. So they already had the majority of this data, but they didn’t want to take a look at my data, which was more complete, because we obtained data from other medical associations throughout the country: from the Royal College of Physicians and Surgeons [of Canada] in Ottawa, from the various provincial medical associations, from the various colleges, and from the various medical alumni associations from the various universities that have medical programs. And so I would have expected that they would have asked me for the copy of the data so that they could properly debunk it, and that simply never took place.
There were other media that got involved—international media [Exhibits VT-3q to VT-3s]. So Reuters from the United States, Associated Press [sic] [Agence France-Press (AFP)], and even the Australian Associated Press put a big red cross across my letter to the Canadian Medical Association saying it was an unproven conspiracy.
Again, I was contacted by Reuters but in a very accusatory tone. I was not contacted by either of the Associated Press news outlets.
There was a big story that was carried in Global News [Exhibit VT-3t]. And I’d like to point out that Ashleigh Stewart did contact me, but she contacted me in a very accusatory manner, really accusing me of harming families, of making things up. And so I tried to answer her questions initially, but as her accusations grew stronger, I simply said, “Look, I don’t want to talk to you anymore” because I understood that she was writing a hit piece and she didn’t ask to see my database.
And so in the graphic that was used by Global News, I want to draw your attention: in the background, there are photos of the deceased doctors. And so on the red, behind the bird from Twitter, are actually the pictures of the deceased doctors, and then they made this graphic with this Pinocchio-like figure made out of a stethoscope. And the article is titled, “Kraken, Elon Musk and dead Canadian doctors: Disinformation surges three years into the pandemic.” And in this Global News article, they state that Global News determined the cause of death of 48 of these doctors, and they talk about cancer and heart attacks and accidents and suicides.
Now, when I had this discussion before this article was published, I asked the reporter if she had any autopsy reports to justify her views and her accusations. And she was evasive and she said, “Even if I had autopsy reports, I wouldn’t give them to you. I wouldn’t share them with you.” And in this newspaper article, there is no indication that there are any autopsy reports to substantiate Global News’s claim that they were able to determine the cause of death of 48 of the 80 doctors.
[00:45:00]
In order to determine the cause of death, you must have an autopsy, and so what Global News did was they read the obituaries, and this was the extent of their investigation. They claimed they contacted some of the families, and so whatever the information the families shared with them. But there is no indication that they had any information about the autopsies of any of these doctors.
In this article they also say that while the efficacy of the vaccines is under debate, their safety is not. And so, again, this is the statement that the safety of vaccines is not under debate—is not debatable. They go on to say that 95 million vaccines were administered and only 0.01 per cent resulted in a serious adverse reaction and that there have been no deaths linked to the vaccine. I believe that they’re referring to Health Canada and their adverse event reporting system.
And then, of course, there are the smears and personal attacks. They say, “Meanwhile, Makis continues to promote conspiracy theories online, most prominently on alt-right website Gettr.” And I had an account on Gettr. Gettr is an alternative to Twitter. I did not see Gettr as an alt-right website, and I certainly did not promote conspiracy theories online, so I saw this as defamation by Global News.
So, you know, I continued despite these attacks. I continued. We continued to assemble our database. And I sent two more letters to the Canadian Medical Association. Really, I didn’t expect any more response at this point, but I did it to simply document that, yes, I did try to contact the Canadian Medical Association. I gave them an update when it was 132 doctors [Exhibit VT-3k]. And at that point, we were able to calculate an excess mortality of physicians in 2022, which was 53 per cent excess mortality compared to 2019. And I sent one more letter on August 13, 2023 [Exhibit VT-3l], when it was 180 sudden deaths. And, again, I did not receive any response from the Canadian Medical Association.
I sent these letters to both Premier Jason Kenney and Alberta Premier Danielle Smith. I did not receive a response from their offices. And also to the Alberta Minister of Health Jason Copping and Alberta Minister of Health Adriana LaGrange, and I didn’t receive a response from that office, either.
So this is the graph that I appended to my last two letters which contains the numbers from our database of the physician deaths, over time, going from 2019, 2021, and ’22. And you can see a clear trend of a steady increase in physician deaths. And, really, the deaths are clustered in the younger physician population. We have calculated— And you could see in the physicians under the age of 30, if you look at 2019, there was one death; 2020, there were zero deaths. And in 2022, there were six deaths. If you average 2019 and ’20, you get half a death a year. Now you’ve got six deaths in 2022. That’s roughly about an 1100 per cent increase in mortality in the youngest doctors. You know, you see a similar pattern in doctors under the age of 40, under the age of 50.
And so, you know, this database is very robust. You know, the database that I gave to the NCI is about 2,300 Canadian doctor deaths over the period of 2019 to 2022. And honestly, you know, I don’t know what else I could have done. I did everything I could to alert the proper authorities on this issue and I was ignored, I was ridiculed, I was insulted, I was smeared in the mainstream media, I was viciously attacked, and I was defamed for my efforts.
Shawn Buckley
And most surprisingly, no one asked to look at your database.
Dr. William Makis
No one has asked to look at the database.
Shawn Buckley
To me, that’s the most interesting part about this, Dr. Makis, is just you went through all this trouble to create data. And we’ve asked you for it and thank you for sharing it. And so everyone can look at it. But it’s curious that all this effort undertaken to debunk this without looking at the data. That’s what I find very interesting.
Dr. William Makis
And I can tell you that this has taken a lot of my time over the past year and a half, and my volunteers have spent hundreds of hours putting this data together. You can see the data is extensive. And they have asked me to keep them anonymous because they are not comfortable sharing their names publicly,
[00:50:00]
and so I’ve honoured their request, but I have shared this database.
And so I would just like to close out this section with a couple of interesting observations: I was a longtime member of the Canadian Medical Association. I still receive the Canadian Medical Association Journal, which I receive a copy every single month. And I look at the journal fairly quickly. And in the April edition I noticed that the entire back cover of the Canadian Medical Association Journal was a Pfizer advertisement [Exhibit VT-3o]. And so I think that was relevant to note in my presentation that the Canadian Medical Association accepts advertisement money from Pfizer.
Recently, just a few weeks ago, the Canadian Medical Association held a health summit—an annual health summit—and the keynote speaker was Mr. Timothy Caulfield. And the keynote presentation was about “the spread of health misinformation” which “poses a genuine threat to Canadian health. But health providers can fight back. In this health summit presentation, [hear] from best-selling author Timothy Caulfield on the importance of debunking false and misleading health messages.” I thought this was an interesting thing to note that the individual who started the media campaign to smear me and to kill the story—as the Toronto Star story said, that they wanted the story of Canadian doctor sudden deaths killed—is giving the keynote presentation at the Canadian Medical Association summit just a few weeks ago.
And, you know, the Canadian Medical Association now has a new president, Dr. Kathleen Ross. This is a family doctor from British Columbia. She just took over on August 16, 2023. And on August 17th, she’s posted a picture with Mr. Timothy Caulfield, and she says she’s excited to listen to his talk on fighting misinformation in health care at the Canadian Medical Association health summit.
And again, I’m a strong believer of disclosing conflicts of interest. And so I wanted to point out that Mr. Timothy Caulfield is a fellow of the Pierre Elliott Trudeau Foundation, and he also runs a social media project that has received federal funding. And this federal funding is to promote vaccination confidence. This social media project is called ScienceUpFirst, and it has been given $2.25 million as an investment, announced by the federal Minister of Health, Patty Hajdu, through the Immunization Partnership Fund. And this fund supports projects that encourage vaccine acceptance and uptake.
And so, in conclusion, I would just like to encourage— I’d like to encourage everyone to look at the data for themselves. I was more than happy to have the data analyzed. I believe there’s a— To my analysis, I believe there’s a very strong signal of excess deaths of Canadian doctors, which really is very significant after the rollout of the COVID-19 vaccines starting in December of 2020.
Shawn Buckley
Dr. Makis, did you notice, because you’ve been analyzing this data— So can you tell us, kind of temporally, was there an uptake— With COVID, was there any correlation between the rollout of the first shot, the second shot, boosters, anything like that? Did you see anything that kind of correlated with any of those events?
Dr. William Makis
There is a mild increase in excess mortality in 2020. Now, of course, it would be ideal to have data going back maybe five years, maybe 10 years, and to compare to longer term baselines. And honestly, I simply didn’t have the time or the access to that kind of data, so the best we could do was compare it to 2019.
There seems to have been a slight increase in 2020, but you see a significant increase in ’21 and even a bigger increase in 2022. And again, I would encourage anyone with expertise in data analysis to analyze this data to see if there is something that—what I had seen.
I do believe, also, that there are spikes in deaths that cluster right around the rollout of the booster shots. So the first booster shot rollout: there seems to have been a spike in deaths just after the rollout of the first booster shot and the second booster shot, as well.
[00:55:00]
But I believe there is a very strong safety signal. I’ve been extremely disappointed that the Canadian Medical Association has ignored it. But I’m extremely pleased that I’m able to provide it to the public through this forum.
Shawn Buckley
Okay, Alberta government. This is interesting. So we have the Medical Association deleting information from their website—and the Alberta government. And it’s fair to say, if the Wayback Machine didn’t exist, you wouldn’t have been able to recover some of this stuff.
Dr. William Makis
That’s correct.
Shawn Buckley
Tell us how you became interested in this and what happened.
Dr. William Makis
You know, I had been tracking— When I was censored from Twitter, I was tracking all kinds of data. I was tracking the Canadian doctors’ sudden deaths, but I was also tracking the data from the Alberta government website, from the BC government website, from the United Kingdom, from Australia. And the data was showing that, over time, the double vaccinated were filling the hospitals. And, you know, there was this push about the “pandemic of the unvaccinated,” and the data just didn’t support the claims that there was a pandemic of the unvaccinated in 2021 and 2022. It really showed that it was the vaccinated who were filling the hospitals.
But I was actually launching my Substack, and I wanted to launch my Substack with something substantial. And I did an investigation into the Alberta data, and I used the Wayback Machine, and I went through the data very carefully. And what I found was truly shocking, and so I wanted to share some of that tonight.
Shawn Buckley
Before you do, I’ll just let the people watching— When we’re saying Wayback or Wayback Machine, all that is, is it’s a service that copies websites periodically. And so let’s say there’s a website that there used to be a page on, and you go back and it’s missing. Well, you use a service like the Wayback Machine, and they’ll go, “Oh, yes, well, six months ago we copied that page and here’s the page.” So it’s a way of accessing old website pages that have changed or have been taken down.
Dr. William Makis
And, fortunately, for the Alberta.ca government website, which published vaccine outcome data, there were snapshots taken several times a day. And so there are thousands of these snapshots in the Wayback Machine that people can go and verify themselves. And so I’ll start my presentation on that.
So on June 3rd, 2021, the Alberta government put a new section on the Alberta.ca website and it was called “Vaccine Outcomes.” And the “Vaccine Outcomes” had tables of data and graphs. And one particular data set that grabbed my attention that I had seen many times before, and it was very interesting, and I wanted to see how that data set had evolved over time. It was a graph called Figure 11 [Exhibit VT-3u]. And Figure 11 was data that showed time from the first dose and second dose of the COVID vaccine to COVID diagnosis, and it was by age group. And so on the y-axis you have how many people are getting infected with COVID-19, and on the x-axis you have how long ago did they have their COVID vaccine.
And so you see these first three graphs on the left: these are people who had one vaccine. And you see there’s a lot of infections initially, and then the infections sort of go down, suggestive of protection. And on the second group of graphs, these are the double vaccinated. And you see there’s very few infections, very few hospitalizations, and very few deaths. And so as the government started putting out this initial data, the data was showing that the two-dose vaccine was protective against infections, hospitalizations, and deaths.
Now I show a set of graphs on the right to show how this data evolves over time, month to month, from July 2021 to August, September, October, November, and December. And these are the double vaccinated. And what it shows is specifically COVID infections in the double vaccinated.
As time goes on, the double vaccinated are doing worse and worse and worse. They’re getting more and more infected. And by December, you see very large numbers of infections in the double vaccinated. And it seems to be worse the longer ago you’ve had your second vaccine dose. So if you’ve had your second vaccine dose six months ago, you’re really doing quite badly, even compared to the people who’ve had their second vaccine dose recently.
[01:00:00]
So to me, this was already indicative that the double vaccinated, there was something wrong. Something had gone wrong with the vaccine, and their immune systems seem to be damaged over time, and this damage seemed to be getting worse as time went on.
By January of 2022, we are in the middle of the Omicron BA.1 outbreak, and this is the last data set that the Alberta government would publish. And there’s a huge spike of COVID infections. You can see the graph on the left: this is the double vaccinated. And there’s a huge spike of infections: thousands. Thousands of infections in the double vaccinated and specifically individuals who’ve had their last dose five, six, or seven months ago, and they’re doing really quite badly. In fact, they’re the ones driving this outbreak, this Omicron BA.1 outbreak. And there’s a cluster in the hospitalizations and deaths, as well, although it’s not as prominent.
And if we compare how it started—how the double vaccinated looked in June of 2021 and how the double vaccinated looked in January of 2022 [Exhibit VT-3v]. These are infections in the double vaccinated. You can see that the double vaccinated are doing extremely badly. Thousands of them are getting infected with COVID-19. There seems to be no protective effect from the vaccines.
Shawn Buckley
And Dr. Makis, how does that compare with the unvaccinated? Because one factor could also be time of year, right? We, northern hemisphere, tend to— I call it low vitamin D season where we get more sickness in the winter months than we do in the summer months. Is there a comparison there?
Dr. William Makis
That’s coming on the next set of graphs, yes.
And I just wanted to point out that this data had actually been shared internationally. It was all over Twitter. People were sharing it, and it was deleted. This figure was deleted by the Alberta government from the Alberta.ca website on January 14, 2022, and this data was never released again. So we never saw this data again.
Shawn Buckley
So was there any explanation as to why they would delete data? Because it certainly seems strange that here you have taxpayer-funded people putting out what should be as reliable as they can be, basically, data, while we’re in the middle of a pandemic. It’s of public interest. Did they give any explanation as to why they would take data down? So it’s not that they even stopped publishing, but they took data down they’d already put up.
Dr. William Makis
That’s right. And I want to point out that this data had been released daily. So every single day this data was updated, and it just disappeared from the Alberta.ca website on January 14th, 2022. As far as I’m aware, there was no announcement made on why this data disappeared on January 14th.
The next data set I’d like to show is Figure 10 [Exhibit VT-3v]. Again, this is in the same section: “Vaccine Outcomes.” All of this data is in the “Vaccine Outcomes” section. This is just a different figure showing a different way that the data is formatted.
Figure 10 showed case rate: so COVID infection rate per 100,000 population by vaccination status. So as you brought up the question of, well, how does this compare to the unvaccinated?
This is the data set that compared the double vaccinated to the single vaccinated to the unvaccinated. And I’m showing here a graph from December 1st, 2021. And the graph really shows that the unvaccinated throughout all of 2021 seemed to have been doing poorly. There was some protective effect with one vaccine dose, and then there was a significant protective effect with two vaccine doses. Again, this is what you would expect if the COVID vaccines were protective. You would expect a much lower infection rate in the double vaccinated compared to the unvaccinated. And that’s what the data showed initially in these graphs.
And so, again, when you look at the Omicron BA.1 outbreak in January of 2022, this data changes drastically [Exhibit VT-3v]. And what you find, especially on the figure on the right at the end of January, is that the double vaccinated are getting infected at the highest rate of all groups. And it’s basically double the rate of the unvaccinated. And so once again, to me, this is evidence of immune system injury in the double vaccinated
[01:05:00]
where they are getting infected with COVID-19 at twice the rate as someone who is unvaccinated.
Interestingly, at some point in January, the government added data on the triple vaccinated. So you will see it as a purple line, and it is labelled as three doses. And initially it seems that the triple vaccinated are doing the best, that they have the lowest infection rate of all the groups, and they seem to be getting this protection that we were all told that the vaccines would provide and that the booster shots would provide. And even during the initial Omicron outbreak in January of 2022, the triple vaccinated are doing the best, which is why I feel—again, I’m just hypothesizing—that the government allowed the data to continue being published despite the fact of how poorly the double vaccinated were doing.
Now we move on to March of 2022 and, again, something has changed in the data [Exhibit-3v]. And what has happened was the triple vaccinated now have the highest infection rate of any group. And so while the Omicron BA.1 outbreak in January was driven by the double vaccinated who had the highest infection rate with COVID-19, now it is the triple vaccinated who have the highest infection rate. And we were actually heading into another wave of COVID, and this was the Omicron BA.2 wave that was going to happen in March, April, and May. And you could tell that the triple vaccinated are actually leading this wave with the highest infection rate of any group. In my interpretation, this is evidence of COVID booster failure. This failure seems to occur in middle of February of 2022, when the triple vaccinated take over as the group that has the highest infection rate of all the other groups.
And then—
Shawn Buckley
So I’m just going to stop you so that people can understand the chart. So you’re really looking at the right-hand side of this chart—
Dr. William Makis
That’s right.
Shawn Buckley
—in February ’22 where the triple vaxxed takes over. Now, what’s interesting is just looking at all of this—and part of this was on a different slide—is at the beginning, the unvaccinated are doing worse.
Dr. William Makis
That’s right.
Shawn Buckley
And then the vaccinated. But then, let’s say, when we move a little over, two-thirds to the right, the double vaccinated are really doing poorly here. And then by the time we’re almost at the end of this chart, I mean, the unvaccinated are doing really well, and now it’s the triple. So your explanation is that as time goes by, the vaccines are creating a problem. Because as time goes by—people—the more shots you have, the worse you’re doing. Is that what the data is showing us here?
Dr. William Makis
Exactly, and so you will see the double vaccinated are doing really poorly in the January outbreak, but then the government is rolling out booster shots during this time. And so, as a little bit of time has gone by with the booster shots, now you start seeing the triple vaccinated are doing very poorly— And they shouldn’t. You know, you shouldn’t see this if the booster shots were protective. You know, the triple vaccinated should be doing better than the unvaccinated and better than the single and double vaccinated. And that’s simply not what the data is showing.
And that is—
Shawn Buckley
And this is just showing us COVID infections. It’s not showing us other health outcomes also.
Dr. William Makis
That’s right. So it’s not showing us hospitalizations or deaths. It’s simply showing us infections.
But again, you know, to my estimation and assessment, the triple vaccinated shouldn’t be getting infected at the highest rate. I mean, that is simply contrary to what the boosters are supposed to do. And so, you know, I would have loved to have seen more of this data. The reason why I put this slide on March 22nd, 2022, is because this is the last slide that the Alberta government would ever release. They deleted this Figure 10 data, and it was never seen again. It was deleted on March 23rd, 2022.
The next data set I would like to show is a table—this is Table 2—and this is COVID case outcomes in Alberta by vaccine status. And now we are looking at hospitalizations: those currently hospitalized and how the total number of hospitalized breaks down by vaccine status.
[01:10:00]
So you could see how many have had three doses, two doses, one, and unvaccinated.
And so you will see that even in March of 2022, the triple vaccinated made up the biggest portion of the hospitalized individuals. And the total vaccinated were—72 per cent were vaccinated in the hospital and only 28 per cent were unvaccinated.
What is interesting, however, is the trend over time. And so when you look at the trend, by the time you get to July of 2022, now the triple vaccinated make up 50 per cent of all the hospitalizations. And all of the vaccinated, as a group, make up 81 per cent of the hospitalizations [Exhibit VT-3w]. The unvaccinated make up 19 per cent. And you can track— If anybody wants to go use the Wayback Machine, you can actually track this trend every single day from March until July of 2022. And you can see that the vaccinated are doing worse and worse, but it is really the triple vaccinated who are flooding the hospitals and in ever-increasing numbers.
And on July 21st of 2022, the Alberta government deleted this data set and did not release it again.
Shawn Buckley
Right, so you had mentioned earlier, we were getting public messaging that basically the unvaccinated were the ones filling up the hospitals and the ICU [the intensive care unit]. And what you’re showing here is for Alberta, the provincial data doesn’t bear that out at all, that messaging.
But one thing that I’m wondering—that would be helpful to even make this more meaningful—is an understanding, well, how many people are vaccinated? How many people have one dose? How many have two? How many have three? And what percentage of the population is unvaccinated? Because the earlier charts were per 100,000, so we actually had a good comparison. Were you aware of that data? Like, I’m just wondering if that would help us with a kind of more meaningful analysis of percentages in the—
Dr. William Makis
Yes, I’m going to show— I don’t have it for Alberta here, but I will show data from British Columbia that’ll sort of give you a better idea of that.
Just to continue on, you know, there was Table 7, which showed those who were in the intensive care unit. And again, the trend shows that, you know, back in March, the vaccinated made up a total of about 48 per cent of those in the ICU, and that rose to 69 per cent by July. And so this data was deleted.
All the data that I’m mentioning now was deleted at the same time: on July 21st, 2022. So Table 2; Table 7 was also deleted.
And then finally, this is the COVID death data [Exhibit VT-3w]. So this is who is dying from COVID-19. And when you look at March, 68.9 per cent of who were dying were vaccinated. That number rises to 83.4 per cent of those who were dying are vaccinated [July 20, 2022]. And this was a trend that really worried me. And so that, you know, the vast majority of the deaths were actually in the vaccinated. And you could see, if you look at the three doses with condition, you could see that that number rises from 35.3 per cent, it rises to 61.1 per cent. So it is really the triple vaccinated that are driving the COVID deaths.
And, you know, I would go as far as to say that this is not just evidence of vaccine injury in the triple vaccinated; this is actually evidence of vaccine injury leading to death because these are deaths from COVID-19 in the triple vaccinated.
And at this time, the triple vaccinated population was about 38 per cent, and they were making up 61 per cent of the deaths. And so, you know, people can verify this, that the triple vaccinated were dying in disproportionate numbers to their prevalence in the population. And so this data was deleted on July 21st by the Alberta government, as well.
Shawn Buckley
I’m wondering, Dr. Makis, just looking at the chart on the right about the deaths: it’s striking, actually, how few deaths there are where somebody doesn’t have another condition. And I’m wondering if that speaks to, you know, COVID not being that dangerous if you don’t have a different condition that’s affecting you. Is that wild speculation or could there be something to that?
[01:15:00]
Dr. William Makis
No, you’re absolutely right. I mean, when you look at the— Again, if people want to focus on the three doses with and without condition, you could see that with no condition, in March, the deaths were 0.8 per cent. It rises a little bit to 1.9 per cent, but the numbers are very small. Whereas, with condition, there is a dramatic rise over time from 35 per cent to 61 per cent. And so this was, to me, very, very concerning data. And I would have loved to see more of this data. And it was deleted on July 21st, and we never saw this data again.
And I would like people to remember that we’ve had a second booster rollout. So we have people who are quadruple vaccinated in Alberta—thousands of them—and we also have thousands of people who are five-times vaccinated, and the Alberta government has released no data on how those are doing.
Shawn Buckley
Would I even be correct in suggesting— I mean, this here is March 31st and then July 20th, 2022, which— And July 20th is the latest data, but we’re not talking about a long data set at all. Like, wouldn’t I be correct that, I mean, even if it went to today, we’re still just talking short-term for these types of treatments?
Dr. William Makis
That’s right, but when it comes to immune system injury, you can see dramatic effects on the immune system over a matter of months. And so you could actually see dramatic differences in how the double, triple, or quadruple vaccinated are doing—even just over a course of six months, twelve months.
And I think this data was absolutely crucial. It was crucial for Albertans to be able to make informed decisions—an informed decision of whether to take the third vaccine or the first booster shot or the second booster shot—and to see how people were doing. Were they doing better? Were they in the hospitals? And I can tell you, this is the last data set of vaccine status of people in the hospital that we have. As of July 21st, 2022, we have no data from the Alberta government as to who is in the hospital, what is their vaccine status, and how they’re doing.
I wanted to show for comparison that it wasn’t just the Alberta government that was deleting data, it was the British Columbia government, as well. And here, the British Columbia government was putting out these nice graphics as to the hospitalizations, intensive care, and deaths. But they also break down what portion of the population is triple vaccinated, double vaccinated, unvaccinated [Exhibit VT-3w]. And so you could actually compare to how it compares to the population.
And I’d like to point out that this is the last data that the British Columbia government ever put out. This is July 16th of 2022. And the deaths— The vaccinated make up 89 per cent of the COVID-19 deaths. And it is, again, driven by the triple vaccinated: 77 per cent of the deaths are triple vaccinated. And if you look at all the way to the left, it shows you what proportion of the population are the triple vaccinated. They are 52 per cent of the population, but they’re making up 77 per cent of the deaths.
And so, if you had a vaccine that simply did nothing and didn’t work, you would expect 52 per cent of the population would be having 52 per cent of the deaths. And in fact, they have a disproportionately higher percentage of deaths. And again, I interpret this as vaccine injury in the triple vaccinated leading to death.
And so this was the last data set that was put out by the British Columbia government. The BC government deleted this data set on July 28th. And I would like to make a comparison to the Alberta government in that the BC government actually put out a press release stating that they were stopping reporting of this data—case outcomes by vaccination status—that that they would be removing this data. And they put out this press release and the explanation they gave was that the data had become “hard to interpret.” And compare this to the Alberta government: the Alberta government did not put out any press release when they deleted their data.
Shawn Buckley
It’s an interesting explanation, isn’t it? “Hard to interpret.” Because, you know, what does that mean and why would that be an excuse for deleting data?
Now, do you know what BC— Because they were helpful to publish the percentage
[01:20:00]
of people that were triple vaccinated and double vaccinated and single and unvaccinated. Did they ever publish a breakdown of, you know, age groups? So when we have that 52 per cent is triple vaccinated, you know, I wonder if more of those were of an older age group because people in care homes and stuff like that couldn’t avoid it. And I’m just speculating. But was there ever any breakdown that way, which would also be helpful for people analyzing data?
Dr. William Makis
I don’t believe so. I’ve never seen any breakdown by age of this information.
Shawn Buckley
Yeah, it’ll be interesting when the data finally is publicly available and what people like you will discover going forward, so—
Dr. William Makis
And so that sort of brings to conclusion my presentation on the data deletion by the Alberta government.
One other thing I wanted to mention was that I believe that publishing this data would have been the responsibility of the public health chief, Dr. Deena Hinshaw, and her office. And beyond that, I don’t know what the involvement of the Health Minister was or the Premier’s office. But, you know, I believe that this data was crucial for Albertans to be informed and to be informed what the vaccine outcomes are. In fact, I will point out that the government deleted the entire “Vaccine Outcomes” section from the Alberta.ca website on July 21st, 2022. And so really, as an Albertan myself, I could say that we’ve been blind in terms of crucial information to make informed decisions on vaccination.
Shawn Buckley
Now, we’re about to segue into your discussion on cancer. And I wanted to start that by just having you explain something because you’re an oncologist—which means you’re a cancer doctor, for those of you that don’t know what an oncologist is—and you’ve spent most of your career heavily involved in cancer diagnosis and treatment. And one thing that we heard kind of as a theme in the media after we were allowed to go back to hospitals— because remember, you and I both live in Alberta, and I think it was the same for most other provinces—is for a short period of time, we were discouraged from seeking healthcare. And a whole bunch of tests and procedures were cancelled for a period of time, including cancer tests.
And so one of the themes that I’ve heard in the media is, “Oh, yeah, well, our cancer rates have gone up because we weren’t testing early; like we dropped our testing and treatment.” And I know you and I had a conversation on Saturday about this, and I really want you to explain to the public— Because I asked you the question, “Well, is there any truth to this?” What type of pattern, as an oncologist, would you expect if we did stop testing and treatment for a period of time? Would we actually have increased cancer numbers? What would you expect? And if you could start with that explanation because I think that would be really helpful for people to get your opinion on that.
Dr. William Makis
Certainly. So if you stopped screening for and diagnosing cancers for a period of time, let’s say for a period of six months, you would expect the cancer diagnoses to drop in numbers during that time, since you’re not screening people; you’re not diagnosing people. And then when cancer services resumed, you would expect there to be a corresponding rise of cancer diagnoses, and it should be proportionate to the cancer diagnoses that you’ve missed during that time when the services were not available. And then, you know, you could compare that to a longer-term trend to make sure that there’s no other factors involved.
Now, what you would expect to see is, you would expect to see some of those cancers would be a bit more advanced. So most cancers are very slow growing, so you would not expect a drastic change in the staging for a lot of the Stage 1 cancers, Stage 2 cancers. There’ll be a very small percentage of them that might advance to the next stage, and so you would see a slightly more advanced stage at diagnosis. And then, of course, you know, the Stage 3, Stage 4 cancer—Stage 3 might become Stage 4 because the cancer might start to metastasize, and so you would see that. But you would certainly not expect the behaviour of the tumours themselves to be any different.
[01:25:00]
So you would—
Shawn Buckley
Right, and the overall trend— I mean, if you’re not diagnosing for a period of time and then you start diagnosing, you’re going to catch those ones you missed. But overall numbers, you are not expecting to change a whole bunch from the trend just because you stopped testing for a period of time. Did I get that right?
Dr. William Makis
Yes, exactly.
Shawn Buckley
Okay.
Dr. William Makis
And as I mentioned, you know, some Stage 3s will become Stage 4. Some Stage 4s will become a bit more extensive, but, again, the behaviour of the cancers is not going to change. And you would be able to see that, yes, some are a little bit more advanced, but you’re not going to see a big difference, certainly not in a short period of time, like six months, for example.
Shawn Buckley
And it’s important that I’ve asked that because, like I say, the media has messaged that this change in cancer behaviour and change in cancer numbers is explained by us not testing and treating for that period of time that we didn’t. And your opinion, as I understand it, is that the media is not correct in their messaging.
Dr. William Makis
That is not correct. As an oncologist, what I’m seeing in terms of cancers that are being diagnosed and the behaviour of those cancers is unlike anything I’ve seen in my career. And I’ve diagnosed tens of thousands of cancer patients with CT [computerized tomography], with cutting-edge PET-CT [positron emission tomography-computerized tomography]. I was the lead PET-CT radiologist in the province of Alberta, and I’ve correlated with MRI [magnetic resonance imaging] findings, with pathology findings—in tens of thousands of cases—and I treated hundreds of cancer patients as a primary oncologist myself.
What I’m seeing now, since the rollout of the vaccines, I’ve never seen in my career. And I want to go a little bit more into depth about what that means.
I actually didn’t catch on to this phenomenon. I only first saw it as my database of Canadian doctors’ sudden deaths grew. And I started seeing these highly aggressive cancers in young Canadian doctors, and that is where I actually first noticed this phenomenon as it was happening.
So what I bring up here is these are three doctors at the same hospital—Mississauga Hospital, Trillium Health Partners—in Mississauga, Ontario. And these three doctors died within three days of each other: And so Dr. Lorne Segall died on July 17, 2022; Dr. Stephen McKenzie on July 18; and Dr. Jakub Sawicki on July 19th. And this was a few days after the rollout of the second booster shot.
So the fourth COVID-19 vaccine was rolled out; a few days later, we have this cluster of deaths. And the only reason we know about these deaths was because a concerned health care worker had actually leaked internal hospital memos. This was not initially publicized in the media, but there were leaked memos announcing the deaths of three doctors in the span of three days at the same hospital. And once that information was leaked, it went viral and then, of course, the media had to address it and then the hospital had to address it, as well.
And so this was addressed in the mainstream media. And so I have some of the mainstream media outlets: here is the CTV News. And right away the hospital put out a statement and the statement said, “The rumour circulating on social media is simply not true. Their passings were not related to the COVID vaccine. We ask, please, to respect the families’ privacy.” Now, this was a very strange statement to me because there would have been no time to conduct autopsies in these three cases. And so there is no basis in reality for the hospital to make a statement like this, that their passings may or may not have been related to the vaccine.
And then additional information came out in subsequent days and weeks that all three of these doctors had cancer. And what caught my eye was the details of the types of cancer that they had.
Two of the doctors, we had more details on their cancer, and so Dr. Lorne Segall, a 49-year-old ENT specialist, just a year prior, had developed Stage 4 lung cancer, and he had died in less than a year. And Dr. Jakub Sawicki, 36-year-old family physician, had developed Stage 4 gastric cancer, and he had died less than a year. Both of these doctors would have presumably been double vaccinated, and then they would have developed this cancer that killed them in less than a year.
And to me, this was a big red flag because, you know, first of all, gastric cancers and lung cancers in individuals of this young age are unusual to begin with. So right there, you’re already dealing with something that’s quite unusual. But the fact that it killed them in less than a year, to me, was a big red flag that there was something very wrong here.
[01:30:00]
This is not how lung cancer behaves. This is not how gastric cancer behaves.
And again, you may have these situations once every few years in your career. So in my career, I would expect to see a case like this—very aggressive, young person with an aggressive cancer, kills them in less than a year—I might expect this once every few years. Here you have two young doctors, working at the same hospital, developing these extremely rare aggressive cancers: they’re dead in less than a year. You know, it was a red flag for me. This is what got me researching into what’s happening with the vaccinated. Are we seeing cancers? What kind of cancers? And that really started my journey of investigating turbo cancers. And this was the summer of 2022.
I then became aware of other stories. You know, the tragic story of Dr. Joshua Yoneda, who was— I’d mentioned him earlier. This was the medical student, fourth year medical student at UBC (University of British Columbia), and I managed to obtain a lot more information about his tragic story. He was mandated to take two COVID vaccines to be able to continue his medical program. He was perfectly healthy and a few months after he took his second dose, he started having back pains. The back pains got worse. He was diagnosed with a spinal tumour. And initially, doctors felt that it was not an aggressive tumour, that it was treatable and that he would just have an operation and he would be fine. They did the operation and then they discovered that this was an extremely aggressive tumour, very rare. It was a spinal cord tumour, and they really struggled to offer him any kind of treatment, and he died less than a year after diagnosis.
And there were other physicians: Dr. Nadia du Toit from Edmonton, 44 years old, came down with an extremely aggressive brain cancer, died in less than a year; Dr. Murray Krahn, 65-year-old internal medicine doctor from Toronto, also developed an aggressive brain cancer and had died in less than a year.
And so at this point, I really suspected that there is something very wrong when it comes to the COVID vaccines and these aggressive cancers that, you know, I had really not seen in my career being this aggressive.
Shawn Buckley
And I just want to be clear because you basically just now walked us through five cases of young doctors that got aggressive cancers and died in a year. I appreciate there was a sixth, but you didn’t have details to share with us. And as an oncologist, you wouldn’t expect to see one of these, let alone five clustered together. Is that what you’re sharing with us?
Dr. William Makis
I might expect to see one. And, again, you do see rare cancers in young people. I don’t want to make it seem that you don’t—you do, but it is exceedingly rare. And these are usually cases that we publish. I have published dozens of such cases: cancers behaving in unusual ways, unusual on imaging. This is something that is so rare you actually publish it in the medical literature to share with other doctors because they may not have seen a case like that in their career.
And so to have five of these cases of— And again, it’s rare for a solid tumour to kill in less than a year. You know, even glioblastomas, which are very aggressive brain cancers, sort of the median survival is 18–24 months. And so to see lung cancer— And again, I’m going to talk about colon cancers, breast cancers, and so on, killing people in a matter of months or less than a year is just absolutely unheard of.
There is a case in the literature for those who want to look at— And I get attacked a lot with the line of attack that there’s no such thing as “turbo cancer,” and there’s no literature about it. And there is actually a case published. Now, this is a case of a 66-year-old gentleman [Exhibit VT-3uu]. It was published by Serge Goldman: 66-year-old man who had two Pfizer vaccines and five months later he presents with enlarged lymph nodes. And so that is the scan on the left. This is a PET scan: a positron emission tomography. These are the types of scans that I used to perform at the Cross Cancer Institute in Edmonton—thousands of these. I had analyzed over 10,000 scans like this at McGill University in Quebec. And he presents—and when you see these little dots around his neck and in his axilla,
[01:35:00]
and in his lower abdomen, these are tumours. These are lymphoma tumours. He was diagnosed with quite an aggressive angioimmunoblastic T-cell lymphoma five months after taking two COVID Pfizer vaccines.
Now, what is interesting about this story is that the doctors had no suspicion that his cancer may have been caused by the Pfizer vaccines. And so they were preparing a chemotherapy regimen for him, and they said, “Look, you’re going to be immunosuppressed with chemotherapy. We’re going to have to give you a Pfizer booster shot to protect you during chemotherapy.” So they give him the Pfizer vaccine booster shot and within days he develops swelling in his neck—big swelling—he feels very sick.
And they did something brilliant, and we’re all fortunate that they did this. They said, “Well, there’s something very wrong. We should repeat the scan. Even though you just recently had the scan, we should repeat the PET scan just to have a more precise baseline before we give you chemotherapy.” So they repeated the scan, and what they found was that the cancer had spread and it had spread to multiple new locations. It had grown in size—it had doubled or tripled in size—and it had spread extensively throughout the body. Now you see new lesions in the neck, in the axillae, in the mediastinum, and in the lower abdomen, and in the groin area. These lesions were not there before—
Shawn Buckley
So, Dr. Makis, according to this, it’s only 22 days between those two scans?
Dr. William Makis
Yes.
Shawn Buckley
How often had you ever seen anything like this?
Dr. William Makis
You would not expect a lymphoma to progress in this way. It simply doesn’t do that. And you know, it’s very fortunate that they decided to repeat the scan because other oncology groups may not have repeated the scan at all. And so it’s fortunate that we have this case where they repeated the scan.
And, you know, as the title says, “Rapid Progression of Lymphoma Following Pfizer mRNA Booster Shot.” And they said, “We have no explanation other than the Pfizer vaccine, the booster shot, for this progression.” And so this case is a stunning example, in my assessment, of what’s being called “turbo cancer.” These cancers that are arising after vaccination that are extremely aggressive, catching oncologists off guard, and they’re behaving unlike cancers that we’ve seen before.
Shawn Buckley
Now, can I just ask you about that term? Because I’m obviously not an oncologist, and so I don’t know what terms are used. But I had never, until recently, even heard the words “turbo cancer” together. Like, to me, turbo is something you put in a sports car to make it go faster, or a diesel truck. So is that a common term that oncologists use or is this a term that’s just come up to explain something that’s new?
Dr. William Makis
No, so this is a word that’s not used by doctors and, certainly, I would not have used this term. It’s not a medical term. It is a term that has arisen in the population. This is how these cancers are referred to by people on social media because of the aggressive nature of these cancers.
Shawn Buckley
Had you ever heard that term prior to the COVID-19 vaccines being used?
Dr. William Makis
No. No, I’ve never heard this term before. And, in fact, when you look at my initial letters to the Canadian Medical Association in September of 2022, I referred to “aggressive cancers.” I don’t refer to the term “turbo cancer.” This is a recent term. I did not come up with this term. It had arisen on social media. That’s as far as I’m aware of it. It is not a medical term.
However, there is no term to describe the phenomenon of what I would call COVID-vaccine-induced cancers. Because, really, the cancers that we see after COVID vaccination behave so differently that you really have to almost create a separate class of cancers associated with vaccination specifically [Exhibits VT-3aa to VT-3dd]. I believe we are dealing with a completely brand-new phenomenon.
Shawn Buckley
Okay.
Dr. William Makis
I had done some extensive research in the literature, and I’ve actually published in peer-reviewed literature on one of the possible mechanisms of how these COVID vaccines may be causing these cancers—these “turbo cancers”—and I will talk about that shortly.
But I was contacted by a journalist from The Epoch Times,
[01:40:00]
who asked me, “Look, we would like to write an article about what are the possible causes of turbo cancers, and would you be willing to tell us? And can you supply, actually, some research from the literature to back up the possible mechanisms?” And so I did that, and this article was published on July 28, 2023, in Epoch Times [Exhibit VT-3z]. And I supplied nine possible mechanisms by which these cancers may be arising. I don’t know if we have time to briefly go over those.
Shawn Buckley
Actually, I don’t want us to skip over this at all. So please give us a detailed explanation on this. When you get to the IgG4 publication, I’ll just indicate that’s been entered as Exhibit VT-3hh.
But no, please give us a— You’re the only oncologist we’ve had, and I think part of the difficulty, Dr. Makis, is that when we were running our hearings earlier, this phenomenon was just evolving. And so I’d actually like you to give us a full explanation if you can.
Dr. William Makis
Certainly.
So I’d like to first say that the exact mechanism by which cancers are arising in those who have had at least one COVID-19 vaccine, the mechanism is unknown. So this is theoretical at this point. We have theories on how these cancers may be arising, and there is literature to back up some of those theories. But at this time, the exact mechanism of how these cancers are arising is unknown. So these are nine possible theorized mechanisms by which these cancers may be arising.
The first one is that the COVID-19 mRNA vaccines specifically have a modified RNA. The messenger RNA has been artificially modified to contain a pseudouridine. So instead of a uridine, you’re now replacing it with a methylated pseudouridine, which has been artificially modified. And this was actually— This has come out of the research of Dr. Karikó and Dr. Weissman, who invented the mRNA vaccines, and they had studied these modifications for many years. And they had discovered that if you modify the mRNA in this way, you could actually dampen the initial immune response of the individual receiving the mRNA so that they wouldn’t destroy the mRNA agent right away. It was actually designed to protect the mRNA [Exhibit VT-3ee].
However, what it does is it interacts with receptors on T-cells and other immune cells, called toll-like receptors, and toll-like receptors are involved in signaling. Immune system signaling is the easiest way to explain it. You have binding of these toll-like receptors, and then you have downstream, signaling effects. Well, some of these changes in signaling are actually implicated in cancer formation, and so this is one of the first mechanisms that should be looked at [Exhibit VT-3ff].
The mRNA vaccines, once they get into your body, they actually dampen— They interact with the toll-like receptors on the immune cells, they dampen the signaling of your innate immune system, and they cause disruptions in immune signaling, which could actually, downstream, lead to cancers being formed. So this is one mechanism.
Dr. Seneff had discovered that there is impairment of a different kind of T-cell signaling, immune signaling, called type I interferon, and this type of signaling is involved in cancer surveillance. So I’ve attached a publication to that [Exhibit VT-3gg]. And again, these haven’t been proven to cause cancer in the COVID vaccinated, but these are lines of investigation. These are theories that should be investigated to see if they are causing these cancers.
Next one, number three, is what’s called the IgG4 antibody shift, and this is a very fascinating discovery. It’s a recent discovery that people who have been vaccinated at least two times start producing a different kind of antibody. So initially, you produce what’s called IgG1 and IgG3 antibodies against the spike protein, and these are antibodies that are involved in protecting us against viruses, but also protecting us against cancer.
And so initially, when you get the first mRNA Pfizer or Moderna vaccine dose, you get these antibodies produced. However, once you get the second shot, the body starts to change the composition of these antibodies, and it starts to produce a different kind of antibody called IgG4.
[01:45:00]
And this antibody is involved in immune tolerance. So it is there to actually get the immune system to tolerate this antigen that you’re now being exposed to several times. And if you get the third dose, it really spikes. And the IgG4 really skyrockets, and you get decreased production of IgG1 and IgG3, and you get a massive rise in IgG4.
And I actually published a paper— We published a paper theorizing what this might be doing in the COVID-vaccinated, that it may be implicated in forming cancers. It may also be implicated in autoimmune diseases and autoimmune myocarditis. We published this recently. It has been peer-reviewed [Exhibit VT-3hh].
And when it comes to cancer, what the IgG4 does is, you know— You’ve got the IgG1 that actually coats cancer cells and calls the immune system to come and destroy the cancer cells. But the IgG4 actually blocks that process from happening. So it can bind the IgG1 and actually prevent the immune system from destroying the cancer cell, or it can occupy sites on the immune cells, like the NK [natural killer] cells or macrophages, and then those cells don’t see the cancer cells. And this is called immune evasion of cancers. And so this is a mechanism that has been published in the literature a number of times, and we are seeing these antibodies in the vaccinated individuals.
And so now you’ve got an immune system that is basically trained to ignore cancer cells, and it then provides an environment for cancer cells to start replicating at an uncontrolled rate because there’s nothing to stop those cancers from replicating, from growing rapidly, and from spreading. Now—
Shawn Buckley
And just for people watching this, my understanding is it’s not like all of a sudden, you know, somebody develops cancer for the first time, and it becomes a problem. But actually, cancer is something we deal with from birth onwards, but our immune system deals with it. We have cells that are made to deal with it. So cancer’s actually a normal process; it’s just when it gets out of control.
But what you’re describing is that normal process is potentially being interrupted by these IgG4 cells.
Dr. William Makis
Yes, and so we produce mutated cells, cancerous cells, all the time, as you’ve mentioned, and it’s our immune system that destroys those cells. And that’s why when I refer to cancer surveillance, it’s actually the immune system that’s surveying the body, the whole body, for these cancerous and mutated cells, and then destroying those cells as it sees them. And we have a very intricately beautiful immune system that takes care of all these mutated, damaged, and pre-cancerous cells and destroys them throughout our lives. And so when something interferes with the immune system, and interferes in a major way, then you’re actually removing that shield and then now some of these pre-cancerous cells can actually start growing rapidly and can spread and metastasize throughout the body.
So this is, again, one of the proposed mechanisms—what’s called an IgG4 shift. Because when the body starts producing this IgG4—especially when you’ve had your third COVID vaccine dose, fourth COVID vaccine dose—it seems the more COVID vaccine doses you’ve had, the more IgG4 you produce and the less IgG1 and 3 you produce. So you’re really removing that shield that you get with the IgG1 and 3 protection against cancers.
Then there are other mechanisms that are really worrying. The spike protein has been found to interfere with tumour suppressor proteins, P53 and BRCA1 (B-R-C-A-1) [Exhibit VT-3ii]. Now, BRCA1 is implicated in breast cancer, ovarian cancer, and P53 is involved in a number of cancers. It’s damaged in a number of cancers. And the spike protein seems to interact or damage these tumour-suppressive proteins. Now, again, it has to be shown that, you know, it’s the vaccine spike protein that’s doing it as well, but that is a very concerning issue.
There’s another paper that shows the spike protein interferes with DNA repair mechanisms [Exhibit VT-3jj; 3-vv]. That is problematic. There’s another paper that shows that the RNA could integrate into our genome and that if it integrates in an area that is a proto-oncogene or a tumour-suppressive protein that it can lead to cancer. This has been shown in vitro [Exhibit VT-3kk].
[01:50:00]
It hasn’t been shown in vivo, but again, another very concerning finding from the literature.
And then there’s been a recent discovery by U.S. geneticist Kevin McKernan who actually did sequencing of Pfizer and Moderna mRNA vials. And he was looking for something else, and he actually discovered that there is DNA contamination in those vials—Pfizer and Moderna vials—and that there is actually a high percentage of contamination of DNA plasmids.
DNA plasmids are rings of DNA that contain the spike protein sequence, and it’s actually part of the normal manufacturing process of Pfizer and Moderna. The way they produce these mRNA vaccines is they put the sequence of the spike protein into a ring of DNA called a plasmid. They then insert that plasmid into E. coli bacteria. They grow those bacteria in large numbers, billions and billions of copies. They then extract those plasmids from the E. coli, and they then transcribe that DNA into the mRNA, and then that mRNA is packaged into the vials and sent out as the Pfizer and Moderna vaccine.
Now, in the quality control process, they are supposed to actually enzymatically destroy all DNA so that there is no DNA contamination from the manufacturing process. And what this geneticist discovered—and it has been replicated in several labs since then, internationally, as well—was that there is a high amount of DNA plasmid contamination in these vials, and that up to 35 per cent of the genetic material in the Pfizer or Moderna vials, up to 35 per cent is actually DNA contamination. And that’s potentially millions or billions of copies of these DNA plasmids.
This is concerning because DNA is much easier to integrate into our genome than mRNA would be. And so if you’ve got all this DNA contamination with the spike protein sequence in it, and you have billions of these DNA plasmids that are injected into you, there is actually a significant risk that these plasmids may integrate into your genome. And again, if it integrates in the wrong place—in a proto-oncogene or a tumour suppressor gene area—you can get cancer that way.
And so this is a recent finding, highly concerning. And I’ve included Kevin McKernan’s extensive documentation and sequencing of this, of these DNA plasmids, as evidence [Exhibit VT-3nn to VT-3pp].
Shawn Buckley
And we’ve entered that as an exhibit. It’s just the list of exhibits— Just so that the Commissioners are aware: almost everything that Dr. Makis is referring to from a research perspective, he’s provided to us, and we’ve included it as part of the record.
Dr. William Makis
Now, just the last two potential mechanisms.
When Kevin McKernan discovered these DNA plasmid contamination in these Pfizer and Moderna vials, he discovered that—specifically in the Pfizer vials; not in the Moderna vials, but the Pfizer vials—the DNA plasmid contained additional genetic information in the DNA plasmid. And this additional genetic information sits before the spike protein sequence, and it’s called the SV40 promoter or the simian virus-40 promoter [VT-3ll]. And this sequence, no one knows why it’s there. Pfizer has not explained why the sequence is there in these DNA plasmids. Simian virus 40 causes cancer in humans [Exhibit VT-3mm] and the cancers that it causes specifically are lymphomas [Exhibit VT-3qq] and glioblastomas—brain cancers.
Now, it is of course a portion of that virus. It is not the entire virus. So only a portion of it was discovered. But again, the concern is it’s a promoter. So it is the sequence that could then encourage transcription of an entire sequence afterwards. So again, if this oncogenic piece of DNA integrates into our genome in the wrong place, it could eventually lead to cancer. So this is another concerning finding that has not been explained by Pfizer, and it’s another potential mechanism by which these cancers may be arising.
And finally, there are sequences in the Pfizer vaccine and Moderna vaccine which are called microRNAs. These are non-coding sequences, so these are additional sequences present, which don’t seem to code for anything. But when they are transcribed, they themselves are potentially oncogenic and cancer-causing [Exhibit VT-3ss].
[01:55:00]
So I’ve attached literature concerning all of these potential mechanisms—these nine different mechanisms—and as I’ve stated, it is unclear at this time which of these mechanisms is the one that’s causing cancer, and it may be more than one of these mechanisms that are causing cancers in different individuals.
Shawn Buckley
No, and I appreciate you being fair with us and making it clear that these are just now theories. There’s not enough research. And I also thank you for providing the research articles. For those that are interested, it will all be part of the record and attached to your witness page. So thank you for doing that.
Dr. William Makis
I wanted to summarize the features of these turbo cancers, just briefly. I have documented over 200 of cases of what I believe are turbo cancers in COVID-vaccinated individuals on my Substack. I have documented these cancers in doctors, in nurses, in teachers, in young people, in pregnant women. And my concern here is that these seem to be arising in greater numbers in professions that had COVID-vaccine mandates implemented on them. So these are, again, doctors—had vaccine mandates—nurses, teachers, military, police officers, firefighters, city workers, and so on, and that is where I’m seeing a greater number of these cancers arising.
So the features of these turbo cancers: They present in young individuals. They can present in teenagers, people in their 20s, 30s, 40s. I do suspect that because I focus on younger individuals, then I’m seeing more of these in younger individuals. It is possible that they may occur across all ages.
Shawn Buckley
Can I just clarify, though, because at the beginning of your testimony on cancer, you were saying, you know, you just weren’t seeing this type of thing before. So even though you’re maybe focusing more on young people, is it still a type of cancer you just wouldn’t expect to see in young people?
Dr. William Makis
I would not expect to see this, and I can tell you I have not seen cancers behaving this way in young people before the rollout of the vaccines. I’ve never seen this in my career. So when I write my Substack, I focus on young people because I feel that, you know, these vaccines should be stopped in young people. But it really— You know, I believe that these are probably occurring across all ages.
These cancers tend to present at Stage 4. They present late. They don’t seem to be picked up. You know, I have not seen stories of Stage 1 and then, you know, it progresses extremely rapidly. They seem to be presenting at a late stage—Stage 3 and Stage 4. They have very rapid growth. And whatever the type of cancer it is, whether it’s breast cancer or colon cancer, lung cancer, they grow so rapidly that they always catch the oncologists off guard.
And you will see these stories anecdotally, if you go to GoFundMe. And we’re not seeing these stories from the medical establishment. This is what’s so frustrating, is that doctors are not publishing these cases. We are seeing these cases on social media. We are seeing them on places like GoFundMe, where the patient will tell us what their experience and what their oncologist told them. And their oncologist will say, “I’ve not seen this. This is 10 years of growth in a month or two, you know?”
And so these tumours grow very, very rapidly over a very short period of time. They are highly metastatic, and what I mean by that is that they spread, and they spread to multiple locations in a very short time. So you know, in some of these cancers, like breast cancer or— Let’s take colon cancer. You know, when colon cancer metastasizes, you expect the first metastasis to show up in the liver, for example, and then, you know, you can actually track that; you can actually surgically remove that, and you can deal with it. These seem to spread to multiple locations in a very, very short period of time.
And another feature which is fascinating, which I have no explanation for, is they seem to be quite resistant to conventional chemotherapy and conventional radiation therapy and other conventional treatments. And what you will find— Again, anecdotal evidence, but what you will find is people will say that they had partial response, but then it was very short-lived. And sometimes the patients will say that the tumour didn’t respond at all to chemotherapy or radiation therapy. And that, again, is really quite unusual.
[02:00:00]
And again, something I really have not seen in my career, that you would have tumours that you would expect to respond to conventional regimens and they’re not responding to chemo or radiation therapy.
And then I’d like to briefly talk about what kinds of cancers we’re seeing. That I’m seeing. And I’ve tried to document, at least on an anecdotal level, how common some of these cancer types are. And it seems that lymphoma is the most common one, closely followed by glioblastoma: these are Stage 4 brain cancers. And then breast, colon, and lung seem to be the common ones. I have seen cancers of the hepatobiliary system: these are the gallbladder cancers; these are pancreatic cancers. They also seem to be happening at a higher rate than I would expect. And the leukemias.
Now, the leukemias. What’s fascinating about the leukemias is that they are so aggressive that the time from diagnosis to death can be a matter of weeks, days, or even hours. I’ve reported on my Substack several cases of leukemia where a young person will feel unwell: they will present to emergency; they will have blood work done; and the doctors discover you have leukemia, and they will die a few hours after diagnosis. And this is, again, something that I have never seen in my career. To die in a matter of hours, even days, after diagnosis is something that I have simply not seen. That is another feature that is really frightening with these turbo cancers.
When it comes to fatality, they kill much more quickly than you would expect tumours of their type. And so, you know, the leukemias are particularly aggressive and deadly, as I had mentioned, but typically, you will see a lot of these cancers kill in a matter of three to six months. And the majority of them, it’ll be six to twelve months. And again, you expect patients with breast cancer, lung cancer, colon cancer to live more than six to twelve months. Even at Stage 4, you expect them to live several years. You know, we have those survival charts, the five-year survival charts, and that’s simply not what we’re seeing. These are lethal, and they kill much more quickly than anything I’ve seen in my career.
And so, you know, that sort of concludes my presentation on the turbo cancers.
Shawn Buckley
Now, I know we were planning on doing sudden deaths during vaccination. Could we just do that in a minute or so? Just we’re running a little late, and I’d like to leave this open for questions from the commissioners.
Dr. William Makis
Absolutely. I would just like to mention that we’ve coauthored a paper [Exhibits VT-3jjj and VT-3kkk]. Now, Dr. Peter McCullough has led this initiative. Dr. McCullough is a Texas cardiologist, and he’s been at the forefront of warning about sudden deaths, specifically cardiac-related sudden deaths, after a COVID vaccination—and Dr. Paul Alexander, Dr. Richard Amerling, Dr. Roger Hodkinson, and Dr. Mark Trozzi: a number of us had gotten together, and we’d conducted the largest review of autopsies that has ever been done of sudden deaths of COVID-19 vaccinated individuals. This is now a pre-print on the Zenodo server. It is under peer review.
We reviewed 325 autopsy cases, and we found that 74 per cent of those deaths were either directly caused by the vaccine or there was a major contribution by the vaccine. And these are sudden deaths shortly after COVID vaccination: the mean time to death was 14 days. And so, you know, this has been seen and downloaded hundreds of thousands of times. We submitted this to The Lancet, and Lancet, within 24 hours, removed it from their server. It was being downloaded hundreds of times a minute and I believe, as an act of censorship and to stop this finding from being peer-reviewed and published, Lancet removed our paper from their server. And so, you know, this is now under peer review and I hope that other researchers will— You know, I hope we get this published, and I hope that other researchers will sort of follow on and build on our research.
We’ve done a similar review of—
Shawn Buckley
Can I just stop you there? The Lancet, it was peer-reviewed and they accepted it for publication, right?
Dr. William Makis
It wasn’t peer-reviewed. Now, it had gone through an initial review and so they saw that, you know,
[02:05:00]
this is an extensively referenced, big paper, so it passed initial reviews. They put it on their preprint server and then, 24 hours later, they removed it from their server; didn’t really give a legitimate explanation why they removed it.
Shawn Buckley
And it was being downloaded extensively.
Dr. William Makis
Yes. And as you can see, it’s been viewed and downloaded, you know, several hundred thousand times. But Lancet, in what appears to be an act of censorship, removed this paper from their preprint server.
Now this paper is being hosted on CERN [Conseil Européen pour la Recherche Nucléaire (European Council for Nuclear Research)], on a Zenodo server, which is sponsored by CERN in Switzerland. And so now people have access to it. They can download it; they can read it. We found that the majority of the sudden deaths of COVID-19-vaccinated individuals are cardiovascular. There’s also a large component of hematological, so blood clots. I think it is a fantastic paper. And I think it sheds a light on the phenomenon of sudden deaths after COVID vaccination.
We wrote a similar review and a paper with myocarditis [Exhibit VT-3lll]. We looked at all the myocarditis cases in the literature in those who were COVID-vaccinated. And we found that 100 per cent of the myocarditis deaths were due to the vaccine. This is also under peer review right now.
And so I’d be happy to move on to answer questions.
Shawn Buckley
Let’s open it up to the commissioners, except if you want to comment. In this slide that you just took down, you’re calling for the suspension of COVID-19 vaccines?
Dr. William Makis
Yes, and so if I may just show the last slide. You know, the purpose of me presenting all this evidence and also giving documentary evidence, I feel very strongly about what I’ve seen in terms of the adverse events of the COVID-19 vaccines. And I am calling for the immediate suspension of the use of COVID-19 mRNA vaccines, especially in children of all ages and pregnant women.
Because the sudden deaths that I described, that we have reviewed—autopsy cases of these sudden and unexplained deaths when people are dying in their sleep or they’re collapsing when they’re playing sports or doing a physical activity, out for a jog, or they’re collapsing in the classroom. I’m seeing this in teenagers—in vaccinated teenagers. I’m seeing these sudden deaths in children—elementary school children. I’m seeing these sudden deaths in pregnant women. It is very disturbing to me as a physician to watch these deaths and watch the injuries, as well [Exhibits VT-3xx to VT-3zz; Exhibits VT-3aaa to VT-3ddd].
I believe there is a substantial body of evidence of very serious adverse events, including deaths, caused by or significantly contributed to by the COVID vaccine [Exhibit VT-3tt; Exhibit VT-3rr]. And it is my conclusion that these pharmaceutical products are neither safe nor effective. And furthermore, I call for the immediate suspension of all remaining COVID vaccine mandates, especially in healthcare. And I hope that other physicians will join me and will find their voice and will find courage to stand up for their patients, to stand up for the Hippocratic Oath to do no harm, and to stand up for the ethical practice of medicine in Canada.
Shawn Buckley
Thank you. So I’ll open this up for questions now. But just, you know, you actually calling for a stop of the vaccinations was worth us coming back to and having you comment on that.
So just go ahead and unmute yourself, Commissioner Drysdale.
Commissioner Drysdale
Dr. Makis, thank you very much. It is a very good presentation. There is a lot of pieces to it, so I want to kind of roll back to the beginning and ask some, probably, what are very fundamental questions.
In your opening part of your presentation, you talked about the Alberta Health Services’ mandates to health care professionals. I believe in that slide you talked about how the—or at least you showed—and I’m just taking a look at the slide right now. You showed how Alberta Health Services had made the statement that immunization against COVID-19 is the most effective means to prevent the spread of COVID-19. Do you have any information as to what scientific basis the Alberta Health Services used to make that statement?
[02:10:00]
Dr. William Makis
I have not seen any document that would support that statement from AHS.
Commissioner Drysdale
My second question, again, has to do with the Alberta College of Physicians and Surgeons. How is a mandate of a medical procedure, specifically a vaccine or a biologic—a lot of the testimony we had said this is not a vaccine, it’s a biologic, but be that as it may—how does the mandating of this medical procedure square with the requirement for informed consent?
And before you answer that, I just want to take a look in— The College of Physicians and Surgeons of Alberta, they define exactly what is required to get informed consent. And one requirement is that the person making the decision to take the procedure has to be free of any undue influence, duress, coercion, or anything else that might influence their decision to give informed consent.
So once again, my question is: How does mandating a medical procedure adhere to the principles of informed consent, particularly when your job is at threat? How did the College of Physicians and Surgeons, do you believe, square that circle? It seems to me, in reading it on the face of it, that mandating a procedure with the threat of losing your job is against the, you know, it certainly violates the coercion part of informed consent. Would you agree with that or do you have any more information to add to that?
Dr. William Makis
Certainly. So I would like to clarify that the mandate was issued by Alberta Health Services. It seems to have been issued unilaterally by the leadership of Alberta Health Services. I know that at the time, the media was asking Jason Kenney, the Alberta Premier, for comment, and the Alberta Minister of Health for comment, and they deferred to Alberta Health Services. And so this was a unilateral imposition of a vaccine mandate.
And you can see in the letter of opposition to the vaccine mandates, the health care workers are clearly stating the scientific basis for opposing these mandates. I consider these mandates highly unethical, unscientific. The health care workers documented the hundreds of thousands of injuries in the VAERS reporting system, you know, over 10,000 deaths. And so I found this a gross violation of medical ethics, of the Canadian Medical Association code of ethics.
The mandates came from Alberta Health Services. Now, what’s interesting is that the College of Physicians and Surgeons of Alberta, they did not put a mandate themselves, but they stepped in and they sent threatening letters to doctors who were opposed to these vaccine mandates. And so there’s an additional layer of coercion where it’s not just that you’re being threatened by your employer, that you will lose your job, or, as was stated, that you will be put on unpaid leave. And we know that there were many health care workers who lost their jobs or were forced into early retirement. But now, here you have the College providing an additional layer of coercion and intimidation by saying that we’re aware of your opposition: we’re putting it on your permanent record, and we’re giving you the opportunity to withdraw your opposition to these vaccine mandates. That, again, to me, was a gross violation of everything I know about medical ethics.
Commissioner Drysdale
Well, you know, you make a point that Alberta Health Services unilaterally imposed these mandates. But the bottom line is that the injections were given by physicians or pharmacists or nurses, and they are all regulated under— At least the doctors are regulated under the Alberta College of Physicians and Surgeons. So the Alberta College of Physicians and Surgeons was directly involved in that they weren’t regulating their members to adhere to the principles and requirements of informed consent.
I mean, I don’t know how it is in Alberta, but I know that in Ontario, it’s not just a regulation under the Ontario College of Physicians and Surgeons. But there’s actually an Act that regulates informed consent in the medical profession outside of that. And I don’t know if that’s the way it is in Alberta or not.
[02:15:00]
Do you know that answer?
Dr. William Makis
So it wasn’t part of my presentation tonight, but I am aware that the College of Physicians and Surgeons of Alberta had sent out a memo to all Alberta physicians indicating that they were not to do anything that would create vaccine hesitancy—and that conflicted with providing informed consent. And furthermore, you know, this includes discussion of risks of the COVID-19 vaccines, and informed consent requires that you discuss both the benefits and the risks.
I have run clinical trials in Alberta. You know, we had regulations that we adhere to very strictly. I had to provide to my end-stage cancer patients a detailed assessment of all the benefits—but of all the risks, as well, with whatever pharmaceutical product that I was going to give them. And in the end, there was no coercion. It was completely up to the patient whether they wanted the product or not.
I’m aware that the College put tremendous pressure on Alberta doctors where doctors were not allowed to provide this kind of informed consent to their patients when the vaccines were rolled out—the first two doses, the booster shots. In fact, that remains the case to this day.
Commissioner Drysdale
Yes, I mean, are you aware of the fact that the CDC and the FDA have approved a new COVID-19 vaccine? And it is my understanding that as of this date, the Pfizer documentation on this actually says that they don’t know what the long-term side effects are. They don’t know what all the side effects are, and they’re still examining this. So that’s current as of September 11th, 2023.
If we don’t know all the side effects and the manufacturer is saying within the last week—September 11th, 2023—that they don’t know all the side effects, how is it possible that they knew all the side effects in December of 2020 when Health Canada approved these vaccines for use in the general population?
Dr. William Makis
Well, I will go one step further: On September 12th of this year—this was a week ago—Canada’s public health chief, Dr. Theresa Tam, and chief adviser to Health Canada, Dr. Supriya Sharma, approved the newest COVID-19 booster shot against XBB.1.5 and recommended these vaccines in children as young as six months old and in pregnant women at all stages of pregnancy. And I’ve read the document that shows the safety studies that were done, and there were no safety studies done on this product in regards to children or in regards to women in pregnancy.
And so, to me— And again, I don’t know what to say about this as a physician, that we have our federal bodies—Health Canada, public health chief—recommending pharmaceutical products on which there were no safety studies done in populations like children as young as six months old and pregnant women.
Commissioner Drysdale
Well, I’ve also read those documents, and I wanted to ask you about that because in the Pfizer document, with regard to the new COVID-19 vaccine, it’s my understanding that there were no clinical trials on it and that they relied on the original clinical trial information.
And also, when I read that documentation, I’m just wondering—since I believe you have read it, as well—they list what they believe are all the side effects for children and they don’t mention death in that list. I mean, you’ve talked about death. I’ve heard many other witnesses talk about death in patients who receive the vaccines, and yet death is not a side effect listed in the Pfizer document. Is that unusual that they wouldn’t list— I mean, that’s a fairly serious side effect, I would think.
Dr. William Makis
It is very unusual, and I find it extremely unusual that to date, Health Canada has stated that there have been zero deaths linked to any of the of the COVID-19 vaccines. When in the United States, in the VAERS reporting system, we have something like over 30,000 deaths reported. Now, of course, you know, these should be investigated.
[02:20:00]
And this is the other part of it—that proper investigations aren’t being done; proper autopsies are not being done. And so, you know, this entire process is, to me, very controversial and questionable.
Commissioner Drysdale
Well, Dr. Makis, that brings me to my next question. And you keep talking about the VAERS system. And for our listeners, the VAERS system is a— I would describe it as a voluntary reporting service for vaccine injuries in the United States. But Canada has its own system called CAEFISS [Canadian Adverse Events Following Immunization Surveillance System] and I don’t believe I heard you mention that word. Have you reviewed the data from the CAEFISS system? Is there a reason you relied on the VAERS system rather than the CAEFISS system?
Dr. William Makis
I have been anecdotally informed by a number of doctors who have submitted vaccine injury reports that whatever reports they submit come back rejected. And this is within Alberta Health Services. Their reports don’t make it to Health Canada. And so their reports are rejected at the level of Alberta Health Services, and they’ve been very frustrated. They’ve of course asked me to remain anonymous. They fear retaliation because they are still working in the system.
Basically, I’ve relied on anecdotal evidence that I’ve seen, and I’ve relied on VAERS reports. I’ve also looked to the WHO VigiAccess database as well in my research.
Commissioner Drysdale
Well, we heard evidence from a number of doctors across the country that corroborate what you just said. As a matter of fact, there was one doctor, I believe, who testified in Truro who reported a number of adverse reactions, according to his testimony, and was dismissed, I believe, because of that, or was at least alleged to be dismissed.
But moving on, you talked about a fellow by the name of Tim Caulfield, who is— I think your title that you had in your slide was Canada Research Chair in Health Law and Policy. And I noticed that when they list him, it doesn’t say doctor. Is he a doctor?
Dr. William Makis
No, Mr. Timothy Caulfield is a professor of law at the University of Alberta.
Commissioner Drysdale
How does a professor of law become the Research Chair in Health [Law and Policy] for the University of Alberta and make commentary on medical matters that you, as a qualified doctor, have made comment on?
Dr. William Makis
I honestly— I can’t answer that question.
Commissioner Drysdale
I have another question that has to do with some of the slides that you had up. And I was searching for one of the references you made. And one of the references was in the slide that you had up and I’m just going to read it.
I don’t see a number on your slide, but it says— It’s a quote out of—oh, gosh, I can’t remember—one of the newspapers who were critiquing what you were saying. And the newspaper said, “According to a recent Epoch Times story,” and then it goes, “—an anti-China publication associated with Falun Gong.” And when they referred to Gettr, they said, “a right-wing” whatever-it-was. And it seems that in a lot of these editorials or these commentaries you’ve got, they put these labels on certain things, and other things they don’t comment on.
And for instance, with Mr. Tim Caulfield, they didn’t say, “a professor of law with no experience in medicine,” which would have been consistent with “Epoch Times—an anti-China publication associated with Falun Gong,” which really didn’t have anything to do with the article.
Have you seen much of that, where the media seems to be putting labels on these outlets in order to— I can only guess it was to characterize them a certain way. Have you seen much of that?
Dr. William Makis
Yes, well, I can tell you— I can specify that the reference to the “anti-China publication” associated with Falun Gong, this was the Toronto Star. This was the Toronto Star article by reporter Alex Boyd. And then the reference to Gettr being an “alt-right” website, this is Global News by reporter Ashleigh Stewart.
These are mainstream media publications. I am not alt-right. I don’t see Gettr as an alt-right website. I certainly don’t subscribe to any of these labels, and I see these labels as, really, a smear tactic.
[02:25:00]
It is a tactic to smear me in their article and to really tarnish my reputation and tarnish my credibility, and really tarnish anything that I have to say.
You will notice that there is no reference that I have won 15 scholarships at the University of Toronto, that I have a four-year undergraduate degree in immunology with honours from the University of Toronto, that I have a five-year specialization from the best medical school in Canada—McGill University. There’s never any reference to my qualifications. There’s no reference to the fact that I’m a cancer researcher with over 100 peer-reviewed publications in international medical journals.
And so, you know, I see these as smear tactics, and I believe I was the victim of a smear campaign by the mainstream media.
Commissioner Drysdale
My next question has to do with Table 2 of the information that you are providing from the Alberta government and particularly— Well, it doesn’t matter which one. You have two different versions of it: one from March 31st, the second one from July 20th. But I’m just looking down and it talks about currently hospitalized—three doses, two doses, one dose, unvaccinated. But when I looked down into the notes, the asterisk says, “Table does not include those with one dose.” But one dose is— Am I misreading this? I mean the table has one dose, but the asterisk in the notes to this Alberta government document says that it doesn’t include with one dose. Am I reading that wrong or is that a mistake by them?
Dr. William Makis
I do see that. And I honestly, you know, I took these—these are snapshots from the government website as it was at the time, in both of those times. I don’t have an explanation of why that statement is there.
Commissioner Drysdale
And we heard testimony from other researchers that— And as a matter of fact, the CDC now says on their website that people who have had COVID-19—I can’t remember if it was boosters or injections—have a higher risk of contracting COVID-19. And where I’m going with this question is, again, going back to Table 2: the government says that within 14 days of getting the vaccine, they don’t consider you protected. But if that’s the risk zone in which you might be getting COVID as a result of the vaccine, aren’t they masking—? Is it possible they’re masking those results?
Dr. William Makis
Yes. So what I would like to say about this data that was being put out by the Alberta government is that, you know, I’m taking this data at face value. I, personally, as a physician, have a problem with the designation within the first 14 days after vaccination that someone would be labelled as “unvaccinated.” I know that this happened and that this was part of the problem with the data throughout the pandemic. And I certainly don’t subscribe to that.
And I believe that data manipulation was used to hide a lot of adverse events following vaccination. And we know that, actually, the majority of the deaths happened in the first two weeks after vaccination. And then those injuries and deaths were actually blamed and labelled as “unvaccinated.”
Commissioner Drysdale
Well, didn’t Pfizer actually say in their monograph that you were considered vaccinated within seven days of receiving the dose? I thought— I’m going by my memory, but I thought we had some testimony on that previously. Are you aware of that, Dr. Makis?
Dr. William Makis
I’m not aware of that. But I know that in Alberta, you know, the definition was 14 days. And it is my belief that initially, when the public health chief, Dr. Deena Hinshaw, talked about the pandemic of the unvaccinated—and then similar sentiments were echoed by Dr. Theresa Tam, Canadian public health chief—that this pandemic of the unvaccinated didn’t exist. That it was a manipulation of the data where— And this was one of the manipulations: that people in the first 14 days after vaccination were labelled as “unvaccinated.”
Commissioner Drysdale
Well, I have two more questions. I know Dr. Massie is anxious to ask some questions, but I have two more questions.
Your specialty is oncology, so you’re a cancer doctor, if you want to call it that. My understanding is that
[02:30:00]
the vaccines were tested initially for a period of about two or three months and then they were unblinded, which means that the side that received the placebo then received the vaccine. So they studied these vaccines—these biologics, as some other witnesses testified—for a period of a few months, two or three months at most.
As an oncologist, if I tested cigarette smokers for two months, would I discover that they got cancer from cigarettes?
Dr. William Makis
No. And there is no long-term testing on any of these products, whether it was the first doses or whether it was the booster shots, Pfizer or Moderna. There has been no long-term testing on any of these products, and this is one of the reasons I was opposed to vaccine mandates, to mandating these experimental products: that we had absolutely no data on what the long-term consequences were of mandating this product on all the health care workers, for example. That was just absolutely unconscionable, unscientific, unethical. And that is why I started my presentation with the vaccine mandates that were imposed in Alberta and, really, throughout Canada.
Commissioner Drysdale
Well, you know, talking about pregnant women: I mean, thalidomide was a drug that was prescribed to women in the early ’60s, I believe, and caused significant issues with birth defects. And once again I ask the question: If you were testing thalidomide now on pregnant women and you tested it for two or three months, would you know whether or not you were going to have birth defects on those women nine months later or six months later?
Dr. William Makis
Well, again, the problem is that even the animal studies that they did were, in my view, insufficient. And when it comes to pregnancy— Sorry, that is my cat. When it comes to pregnancy, where I’m really concerned is that there is a blanket recommendation of these products in pregnancy. And I have published on my Substack, I have reviewed the VAERS database extensively in terms of what has been reported, the problems that have been reported in pregnancy, and there are very serious problems that have been documented in the VAERS reporting system.
When you take the COVID vaccines in early pregnancy, there are congenital malformations of the heart, of the brain, of the limbs [Exhibit VT-3ggg]. When you take them in the second trimester, the fetus can stop growing within 24 hours of taking the Pfizer or Moderna vaccine. There are many such reported cases. There’s a cessation of fetal growth that can lead to miscarriages or stillbirths [Exhibit VT-3fff]. And in the third trimester, there are many cases of stillbirth [Exhibit VT-3hhh], of premature labour, of maternal death, death during delivery of the mother or the baby, postnatal deaths [Exhibit VT-3eee] . These are very highly concerning cases, and that’s why I want to see these products stopped. It should not be recommended for pregnant women until there’s much more robust studies done.
Commissioner Drysdale
We also heard significant— And I’m going to ask you this question because you talked about cancers, that there was no screening done for a year or two and that, of course, there was an increase in the number of cancers detected after they started screening again. So they essentially stopped screening for cancers. And my question to you, or at least what I’m wondering about is, we heard testimony after testimony after testimony from medical professionals who said the hospitals were empty, who said that there was nothing going on. We saw commercials of nurses dancing in the emergency rooms. I, myself, had an experience in an emergency room during the lockdowns, and the emergency room and the hospital was empty.
So my question is, how in good conscience did we stop doing cancer screenings with the full knowledge of what the impact that would have when the medical system was not overloaded? At least according to the testimony we had: the hospitals were not overloaded; the emergency wards were not overloaded. And yet we stopped all these preventative measures. And according to your testimony, you’re expecting an increase,
[02:35:00]
or you have seen an increased number of cancers detected, partially because we weren’t doing screening for a year and a half or two years. Have you any insight into how they decided to stop doing those screenings, knowing what the risk was, and knowing that the hospitals were not overloaded in the first place?
Dr. William Makis
Again, I can’t really speak to the decision making. Certainly, I would not have stopped those visits or cancelled those visits, or cancelled the surgeries. There were many surgeries that were cancelled, as well.
I don’t believe it was that long of a period of time. I believe it was a number of months. I can’t tell you exactly the length of time, but I don’t believe it was more than a year.
And in terms of the expected increase you would see, as we would sort of catch up on those patient visits and screenings, again, it does not explain the phenomenon that I’m seeing with these cancers that are arising, and very, very aggressive cancers. And I am seeing this phenomenon in the United States. I’m seeing this phenomenon in the United Kingdom, in Australia, in all the countries that have a high uptake of the COVID-19 vaccine—specifically the mRNA vaccines—and also have high booster uptake. I’m seeing the same types of cancers in these different countries. And these countries, some of them didn’t have, you know, closures or cancellations of cancer screenings or cancer visits, so this is a completely separate phenomenon.
One thing I would like to add is that it is impossible to get good data on the rate of cancers. I’ve tried to get this data. I’ve gone to Statistics Canada. I’ve gone to the Public Health Agency of Canada. You know, I’ve looked at the Canadian Cancer Society. None of these institutions, which should be releasing this data to the Canadian public, none of them are releasing this data. These three institutions put out a report in 2022 where the data only goes up to 2018. So we’re actually not seeing any data—any data—on the incidences of cancer in 2021 and 2022, which is the data that we need to see to be able to assess this phenomenon of these aggressive cancers arising. You know, what is the rate of increase of these cancers and the particular types of cancers, as well?
I mentioned that there seems to be, anecdotally, a huge spike in lymphomas, glioblastomas, Stage 4 breast cancer, Stage 4 colon cancer, Stage 4 lung cancers, but we need broader data from these institutions—Statistics Canada, Public Health Agency—and we’re not getting them.
Commissioner Drysdale
Well, your commentary on that particular item seems to be confirmed by Dr. Denis Rancourt, who testified here three times, and testified a third time because during the first two testimonies, the Canadian data was not available and he had used data from other parts of the world.
But those are my questions, Dr. Makis. Thank you very much for your time and your expertise and your courage to come before this committee.
Dr. William Makis
Thank you very much.
Commissioner Massie
Good evening, Dr. Makis. Thank you very much for this very detailed and, I would say, comprehensive presentation. What you’ve covered actually overlaps with a lot of other stories we’ve got from many other experts. But the emphasis you’re putting— And I will focus my question mostly around the cancer and the potential mechanism for the cancer.
I have some knowledge in the tumour biology: I’ve been trying to develop protocols to fight cancer with gene therapy and stuff like that, so I have some knowledge. And it seems to me that one of the keys in cancer is really the immune surveillance of cancer. And one of the things that I’ve heard anecdotally from people in my surroundings is that some people have had cancer in the past that would seem to have been completely cured for, sometimes, decades. And after their second or third shot, it just went back, and they basically died from cancer in a couple of weeks or months. So how could you actually explain these kinds of cancers that seem to have been completely cured for decades, but all of a sudden are coming back following the immunization with these mRNA vaccines?
[02:40:00]
Dr. William Makis
I would like to state that Professor Angus Dalgleish in London, in the United Kingdom, has made a public statement—exactly what you are mentioning, as well—that he, as an experienced oncologist, has seen a number of instances of cancer patients who had been stable—for example, melanoma cancer patients who had been stable on a certain kind of immunotherapy for many, many years. And then they take a COVID-19 booster shot, and then their cancer just explodes and spreads. And he said other patients who’ve been in remission and then their cancer returns, and it is aggressive and it is much more aggressive than before.
And again, I don’t have an explanation for this phenomenon. You know, again, it’s theoretical at this point. And again, it may have to do with some kind of suppression, immune suppression: that could be why these cancers can suddenly come back, but, again, it’s something that really needs to be researched. And I don’t believe this kind of research is being done because there’s no acknowledgement within oncology, as a medical specialty, that this phenomenon exists or that this phenomenon could even be a problem in the COVID-vaccinated. And so I think this is something that requires research. But it would first require an acknowledgement that the problem exists, that it is something that needs to be researched.
I’m sorry, I don’t really have a theory right now on that phenomenon.
Commissioner Massie
On a follow-up question on that: when I look at your different mechanisms you’re proposing as potential triggers for these cancer, some of them seem to qualify, what I would call, hit-and-run. That is, something would trigger the initiation of the cancer, and then it might take some time before the cancer really flourishes and, in fact, affects the individual up to the point that they will die. So what kind of research would be required in order to really link the occurrence of the cancer to that kind of triggering, which sometimes may or may not leave a trace of the initial event?
Dr. William Makis
Well, you know, I wonder about these events where the RNA is reverse transcribed into our DNA, or this issue with the DNA plasmids potentially integrating. So there would probably need to be some kind of sequencing testing done on people who’ve been vaccinated to see if there have been any integration events.
And I know that this is a concern of a number of doctors: that it’s one thing to have the mRNA persist for a certain period of time and have the spike protein being produced for a certain period of time, and then, you know, eventually the mRNA degrades. Even the modified mRNA—which is supposed to last longer now that it’s been modified with the pseudouridine—it degrades at some point, and the spike production may cease. But the concern is—is this spike protein sequence being integrated, in certain cells, into our genome? And then you’re now faced with a situation where you’re potentially producing spike protein indefinitely, and it’s causing all kinds of immune issues.
And so I would love to see much more research around this problem of this integration of this spike protein sequence into our genome. And I don’t have the expertise in that to really go beyond that. But I think that, for me, that would be an area of really strong interest.
Commissioner Massie
So I understood from your previous answer that, at this point, we don’t gather enough data, maybe, to get a good assessment of the occurrence of this phenomenon in terms of a serious side effect of the vaccination?
Dr. William Makis
I don’t believe the research is being done.
Commissioner Massie
So my question would be:
[02:45:00]
Your best assessment based on what you’ve scanned or the data you gathered, how would you compare that to, say, the occurrence of myocarditis? Is it, like, much lower in terms of rate? Is it same ballpark? Is it higher?
Dr. William Makis
Well, so myocarditis is a very interesting issue because I believe we’ve been lied to by the public health authorities about myocarditis, specifically the incidence of myocarditis in the COVID-vaccinated. I know that public health officials in Ontario, for example, have admitted a rate of one in 5,000. You know, there’s been different numbers published in the literature: one in 10,000; one in 20,000 per dose.
But then you have the studies, like the prospective study in Thailand by Mansanguan, which shows a potential of subclinical myocarditis as high as 1 in 30. One in 30 young boys—you know, the teenage boys. You have the study from Switzerland by Dr. Christian Mueller who had looked at, you know, 800, approximately, health care workers after taking the booster shot and finding some evidence of cardiac damage—and he says it’s mostly mild damage, but some evidence of cardiac damage in 1 in 35.
So there’s a huge disparity in terms of what the public health officials are willing to admit in terms of how frequent these events are and what is happening on the ground. When you look at large databases like the WHO VigiAccess database, which has five million adverse events reported from COVID-19 vaccines, there’s a disconnect there. And so I think when it comes to the cancers, as well, we have a worse situation because there’s actually no admission from any of the public health authorities in Canada or the United States that this phenomenon even exists.
So it’s one thing to have public health officials admit, yes, the vaccines cause myocarditis, it’s rare and mild—and that’s the lie. But there is an admission that it can cause myocarditis; it can cause blood clots. But in the case of cancer, there is no admission by any health authority in the world that this is even a possibility.
I’m sorry, you’re muted.
Commissioner Massie
So, yeah, when you do autopsy for myocarditis, you can find the spike protein in cardiac cells and cardiac tissue and get some sort of reasonable assessment that seems to be a mechanism that linked the two events. But in cancer, what kind of autopsy could you do in order to link the cancer with the vaccine? Can you think of ways that we could actually sort that out?
Dr. William Makis
This is going to be a lot more difficult. I am aware of some work done by Dr. Arne Burkhardt in Germany, pathologist, who has done some staining for the spike protein. I believe he’s done some staining on tumour tissue. Dr. Ryan Cole in the United States, pathologist, has talked about this phenomenon of at least staining for the spike protein in the tumour itself.
And that’s not being done. That’s not being done in Canada. That’s not being done, you know, in the United States by any of the medical authorities, but at least this would be a start. This would be a start: Is there presence of the spike protein in these tumours and how much spike protein is present? That would at least be the starting point for me.
Now again, that may not be sufficient in terms of linking many of these cancers to the vaccines, but at least we could start with that. And unfortunately, that’s not being done.
When it comes to these cancers, I can tell you, we are so far behind in terms of approaching this topic in any scientific way that I feel very alone on this topic. As I mentioned, there’s Professor Dalgleish in London, in the United Kingdom, an oncologist who is also calling for investigations into these types of aggressive cancers. Of course, Dr. Roger Hodkinson, pathologist in Alberta, you know, believes this phenomenon of turbo cancer is happening. Dr. Ryan Cole in the United States, Dr. Arne Burkhardt in Germany, Dr. Peter McCullough in the United States, as a cardiologist.
[02:50:00]
Recently, Dr. Harvey Risch has talked about turbo cancers, as well. But this is a very, very small group of us that are sounding the alarm on what we are seeing on the ground level—at the anecdotal level, really. And unfortunately, the medical community is simply not willing to look at this. Really, similar to the way the Canadian Medical Association is not willing to look at the phenomenon of sudden deaths of Canadian doctors. There’s just no interest in looking for answers.
Commissioner Massie
I have another question. I was really curious about one of the mechanisms you mentioned about microRNA that could actually perturb the gene expression in the cell. Have you looked at some of the data showing that these microRNA can actually be derived either from the plasmid that uses a template to make the RNA vaccine, or is it possible that in the process of generating the RNA, you are generating the short segment? And do we know anything about whether these segments can actually have been shown to be a potential sequence to affect gene expression? Have we done some genomic analysis on that?
Dr. William Makis
I’ll be honest, this is not my expertise. You know, this is beyond my expertise. You know, I’m aware that some of these sequences could act as either tumour suppressors or proto-oncogenes, but this is really not my area of expertise.
Commissioner Massie
So let me get back to immunology because that seems to be one of your expertise. I’m really concerned about the IgG4 potential role in the triggering of cancer because you would actually interfere with normal immune surveillance and you would generate an environment that is conducive to growth of cancer.
So I have two questions here. The first question is, it seems that from the literature, the occurrence of IgG4 increased with the number of doses of the mRNA—at least starting at the third dose and after that it seems to be pretty high: stable high.
So my first question is about these new vaccines that the health authorities are pushing for the fall. And they somewhat changed the message, at least in the States. I don’t know in Canada whether they’re going to use the same spin on it, which is this is not a booster: this is just a new vaccine for a seasonal, if you want, COVID strain similar to flu seasonal vaccine. But it seems to me that if you use the same mRNA technology, it’s another injection that actually should be on top of what you already have. So should that actually further stimulate IgG4 or maintain it at high levels for people that have been previously injected, say, twice, and they decided to get their shot in the next fall?
Dr. William Makis
I believe so. I believe the antigen is almost virtually the same as the initial vaccines that you would have been exposed to the first dose, the second dose, you know, the first and second boosters. You know, they may have made some very minor modifications in terms of, you know, the Omicron XPV.1.5, but it is my understanding that the body would recognize it as just another exposure and that would probably continue driving this mechanism, this IgG4 shift. And really, it’s very interesting that there’s a very minor rise in IgG4 with the second shot. But it is the third shot that seems to make a very dramatic increase in this production of these IgG4 antibodies. And so just continuing along this path, I think, is just absolutely reckless.
And, you know, I see this departure from the word booster as a marketing ploy. Canadians, by and large, have stopped taking booster shots. I believe only five or six per cent of Canadians are considered up to date on their booster shots or have taken a booster shot in the past six months. And so it’s clear that booster shots are unpopular—highly unpopular—even among people who have taken vaccines before.
[02:55:00]
And so I have actually read in the literature—now this is referred to as vaccine hesitancy literature—that they want to actually change the marketing of these vaccines, remove the word booster, and make them appear as annual, updated shots that you would get at your regular doctor visit, just like you would get your flu shot. And they really— It seems to be that there’s this desire to now move towards this idea that these are harmless, annual shots just like the flu shots because the flu shot is seen in the literature as being very successful in the way it was marketed. And the uptake of the booster shots over a number of years: that the marketing involves removing the word booster and now changing the name of these shots as “updated shots” as opposed to “booster shots.”
But they are booster shots. It’s the same antigen. I believe you’re just exposing your body to more of the same antigen. And if you are on this IgG4 shift, I presume that just taking another shot only worsens the situation.
Commissioner Massie
So maybe one last question. I mean, there could be many more, but it’s been a long night.
We started to see in the literature a lot of study around what they call “spikopathy,” which means that the spike protein itself is toxic and creating all kinds of pathology. It could come from the infection with the virus, as well as the vaccine, and it could be a combination of both.
But there is a push, it seems to me, to say, “Okay, in the mRNA platform, the problem could have been the spike protein, but if we now develop other types of vaccine with other antigens, then it’s going to be fine”: In other words, the mRNA lipid [nano]particle platform is fine, is perfectly effective and safe. It’s just maybe the spike, which was not a good idea. But now if we put something else for RSV [respiratory syncytial virus] or any other of this long list of vaccines that they want to shift—I think they want to do flu, as well—then it’s going to be fine because these other potential antigens will not have the issue of the COVID because it was spike.
So what is your take on that? Is it mainly the spike that’s responsible for the issues we’re seeing with these type of mRNA vaccines, or is it also the platform?
Dr. William Makis
I believe it’s the platform. I believe the entire lipid nanoparticle mRNA platform is problematic. And I’ve noticed this same kind of phenomenon in terms of blaming the spike protein of the coronavirus and actually rehabilitating the platform and saying the platform is fine. I’ve seen this talked about with the protein they plan to use with influenza vaccines, for example, that it’s less likely to mutate and it’s not like the spike protein; it’s not going to cause the same problems. I believe the lipid nanoparticle mRNA platform is the problem, and the problem is that the lipid nanoparticles, when they’re injected with mRNA, regardless of the mRNA, they go systemic. And I believe that it is this systemic distribution that is the source of virtually all the injuries that we’re seeing—the vaccine injuries.
Now, of course, the spike protein is highly inflammatory and its expression in the various organs and the distal expression is highly problematic. But I believe that we would see similar kinds of problems with any other protein, whether it’s from influenza or RSV or HIV [human immunodeficiency virus] or CMV [cytomegalovirus]. I know that all these vaccines are planned, and I believe we’re going to see similar proteins because the lipid nanoparticle does not stay in the arm. There’s no mechanism for it to stay in the arm. It very quickly ends up in the bloodstream, is delivered systemically, and I believe that’s where you run into the problems: you’re delivering this mRNA systemically, which shouldn’t be delivered systemically.
Then you’ve got the translation of this foreign protein, and being expressed in tissues that should not be expressing this protein, causing all kinds of immune reactions and just causing immune havoc, which then leads to— You know, you’ve got the myocarditis, you’ve got the blood clots, you’ve got various autoimmune injuries.
[03:00:00]
And, of course, the lipid nanoparticles crossing the blood-brain barrier is a problem, crossing the placenta is a problem. This has not been addressed at all.
And I have seen a presentation by Stéphane Bancel, the CEO of Moderna, saying very clearly, “We’re going to use this same exact technology in all our future vaccines. We’re going to use the same production method, the same manufacturing methods.” And so I believe that this entire platform, this lipid nanoparticle mRNA platform has to be shut down, has to be stopped. There have to be a lot more independent studies, or what have you, before this is ever brought back again. I believe that this platform is the problem. It’s not the spike protein—it is the entire lipid nanoparticle mRNA platform.
Commissioner Massie
Thank you very much, Dr. Makis.
Shawn Buckley
Well, that being all the questions, Dr. Makis, first of all, on behalf of the National Citizens Inquiry, I want to sincerely thank you for coming and testifying. You have provided some information— And perhaps it’s fortunate that your testimony got delayed. We did want to fit you in earlier, but we had scheduling problems. But you were able to share something that you couldn’t have talked about until now. And I think this is going to go down as extremely important testimony, and I think a lot of people watching this are going to be really shocked by what you had to say. And so I sincerely thank you for taking the time and effort to attend at the National Citizens Inquiry and testifying with us today.
Dr. William Makis
Thank you very much for giving me the opportunity to testify.
[03:01:53]
Summary
Dr.William Makis is a Nuclear Medicine Radiologist and Oncologist living in Alberta, Canada.
Dr.Makis fled Communist Czechoslovakia in 1988 through a United Nations refugee camp, grew up in Toronto and obtained a degree in Immunology at University of Toronto, before proceeding with medical training at McGill University in Montreal. Dr.Makis is also a Cancer Researcher with over 100 peer reviewed publications and the Chief of Oncology at The Wellness Company.
Since 2021, Dr.Makis has been voicing concerns about COVID-19 vaccines, vaccine mandates, and the sudden deaths of Canadian doctors and children since the rollout of the mRNA vaccines.
VT-3-Makis-CV 01a-NCI-2023-09-15-CV-Makis
VT-3a-Makis-NCI-Sep18-MAKIS-FINAL-PPT
VT-3aa-Makis-Eens 06b-Turbo-Cancer-Paper01-Eens-Mice
VT-3aaa-Makis-07b-NCI-Children-Injured03
VT-3b-Makis-Tweet 01b-NCI-2021-08-Booster-Failure-Twitter
VT-3bb-Makis-Cavanna 06b-Turbo-Cancer-Paper02-Cavanna
VT-3bbb-Makis-07b-NCI-Children-Injured04
VT-3c-Makis-AHS 02a-AHS-Mandate-2021-08-31-from-AHS
VT-3cc-Makis-Mitsui 06b-Turbo-Cancer-Paper03-Mitsui
VT-3ccc-Makis-07b-NCI-Children-Injured05-Died-some-VAERS
VT-3d-Makis-AHS Mandate 02b-AHS-Mandate-2021-08-31-Calgary-Herald
VT-3dd-Makis-Lam 06b-Turbo-Cancer-Paper04-Lam
VT-3ddd-Makis-07b-NCI-Children-Injured06-Deaths-hidden-VAERS
VT-3e-Makis-Canadian Press 02b-AHS-Mandate-2021-08-31-Canadian-Press
VT-3ee-Makis-Morais 06b-Turbo-Cancer-Paper05-Morais
VT-3eee-Makis-08a-NCI-Pregnancy01-breastfeeding-VAERS
VT-3f-Makis-AHS CTV 02b-AHS-Mandate-2021-08-31-CTV
VT-3ff-Makis-Javais 06b-Turbo-Cancer-Paper06-Javaid
VT-3fff-Makis-08a-NCI-Pregnancy02-fetal-demise-VAERS
VT-3g-Makis-AHS Global 02b-AHS-Mandate-2021-08-31-Global-News
VT-3gg-Makis-Seneff 06b-Turbo-Cancer-Paper07-Seneff
VT-3ggg-Makis-08a-NCI-Pregnancy03-Congenital-Malformations-VAERS
VT-3h-Makis-CPSA 02c-NCI-2021-10-12-CPSA -AHS-Mandate-Letter
VT-3hh-Makis-Makis 06b-Turbo-Cancer-Paper08-Makis
VT-3hhh-Makis-08a-NCI-Pregnancy04-Stillbirths-Mostly-VAERS
VT-3ii-Makis-Singh 06b-Turbo-Cancer-Paper09-Singh-p53-BRCA
VT-3iii-Makis-09a-NCI-Makis-Paper-IgG4-Cancer-Autoimmunity
VT-3i-Makis-CMA 1 03a-NCI-2022-09-03-CMA-Letter01
VT-3j-Makis-CMA 2 03b-NCI-2022-10-15-CMA-Letter02
VT-3jj-Makis-Panico 06b-Turbo-Cancer-Paper10-Panico
VT-3jjj-Makis-09b-NCI-Makis-Paper-Autopsy-Sudden-Death-Vaccine
VT-3k-Makis-CMA 3 03c-NCI-2023-02-18-CMA-Letter03
VT-3kk-Makis-Alden 06b Turbo-Cancer-Paper11-Alden
VT-3kkk-Makis-09b-NCI-Makis-Paper-Autopsy-Sudden-Death-Vaccine-Supp-Table
VT-3l-Makis-CMA 4 03d-NCI-2023-08-13-CMA-Letter04
VT-3ll-Makis-Strayer 06b-Turbo-Cancer-Paper12-Strayer
VT-3lll-Makis-09c-NCI-Makis-Paper-Myocarditis-Vaccine
VT-3m-Makis-Doctor Deaths Excel 03e-NCI-Canadian Doctor Deaths 2019-2023 (as of 2023.06.30)
VT-3mm-Makis-McKernan ET 06b-Turbo-Cancer-Paper13a-McKernan-Epoch-Times
VT-3n-Makis-CMA 03f-NCI-CMA-2022-10-20-CMA
VT-3nn-Makis-McKernan Substack 1 06b-Turbo-Cancer-Paper13b-McKernan-Substack01
VT-3o-Makis-Pfizer 03g-NCI-CMA-2023-04-Pfizer
VT-3oo-Makis-McKernan Substack 2 06b-Turbo-Cancer-Paper13b-McKernan-Substack02
VT-3p-Makis-Toronto Star 04a-2022-11-07-TorontoSTAR
VT-3pp-Makis-McKernan Substack 3 06b-Turbo-Cancer-Paper13b-McKernan-Substack03
VT-3q-Makis-AP 04b-2022-11-25-Australian-AP
VT-3qq-Makis-Butel Turbo Cancer 06b-Turbo-Cancer-Paper13c-Butel-SV40
VT-3r-Makis-Reuters 04c-2022-12-30-Reuters
VT-3rr-Makis-Abdelmassih Turbo Cancer 06b-Turbo-Cancer-Paper14-Abdelmassih
VT-3s-Makis-AFP 04d-2023-01-06-AFP
VT-3ss-Makis-Otmani 06b-Turbo-Cancer-Paper15-Otmani
VT-3t-Makis-Kraken 04e-2023-01-14-Kraken
VT-3tt-Makis-Wiseman 06b-Turbo-Cancer-Paper16-Wiseman
VT-3u-Makis-Tampering 05a-NCI-Alberta-Data-Tampering-Part1
VT-3uu-Makis-Goldman 06b-Turbo-Cancer-Paper-Other-Goldman
VT-3v-Makis-Tampering 2 05a-NCI-Alberta-Data-Tampering-Part2
VT-3vv-Makis-Jiang 06b-Turbo-Cancer-Paper-Other-Jiang-p53-BRCA
VT-3w-Makis-Tampering 3 05a-NCI-Alberta-Data-Tampering-Part3
VT-3ww-Makis-Kyriakopoulos 06b-Turbo-Cancer-Paper-Other-Kyriakopoulos
VT-3x-Makis-Tampering 4 05a-NCI-Alberta-Data-Tampering-Part4
VT-3xx-Makis-07a-Children-deaths-flu-CBC
VT-3y-Makis-Tampering 05b-NCI-Federal-Data-Tampering
VT-3yy-Makis- 07b-NCI-Children-Injured01-VAERS
VT-3z-Makis-Epoch Times 06a-Turbo-cancer-Epoch-Times
VT-3zz-Makis-07b-NCI-Children-Injured02-Children-wrong-vaccine-given
{kind=link}
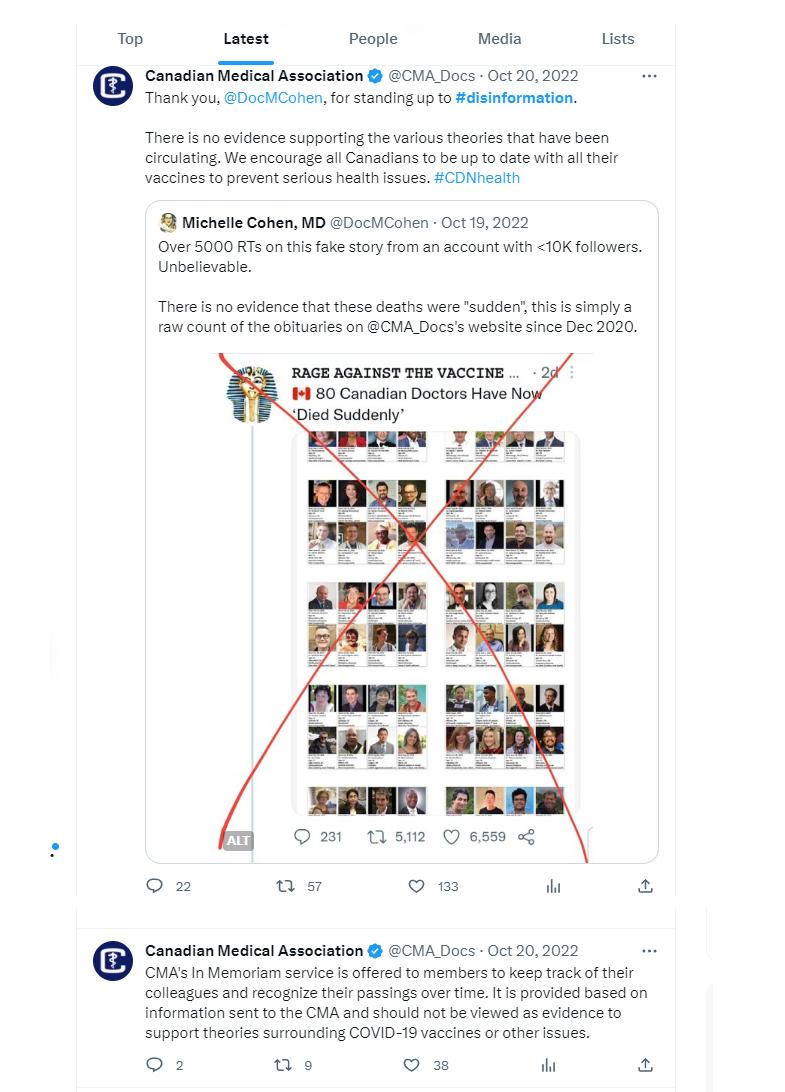{kind=link}
{kind=link}
Follow NCI On Social Media and Podcasts:







